

In-bag manual versus uncontained power morcellation for laparoscopic myomectomy
- PMID: 32374421
- PMCID: PMC7202470
- DOI: 10.1002/14651858.CD013352.pub2
In-bag manual versus uncontained power morcellation for laparoscopic myomectomy
Abstract
Background: Uterine leiomyomas, also referred to as myomas or fibroids, are benign tumours arising from the smooth muscle cells of the myometrium. They are the most common pelvic tumour in women. The estimated rate of leiomyosarcoma, found during surgery for presumed benign leiomyomas, is about 0.51 per 1000 procedures, or approximately 1 in 2000. Treatment options for symptomatic uterine leiomyomas include medical, surgical, and radiologically-guided interventions. Laparoscopic myomectomy is the gold standard surgical approach for women who want offspring, or otherwise wish to retain their uterus. A limitation of laparoscopy is the inability to remove large specimens from the abdominal cavity through the laparoscope. To overcome this challenge, the morcellation approach was developed, during which larger specimens are broken into smaller pieces in order to remove them from the abdominal cavity via the port site. However, intracorporeal power morcellation may lead to scattering of benign tissues, with the risk of spreading leiomyoma or endometriosis. In cases of unsuspected malignancy, power morcellation can cause unintentional dissemination of malignant cells, and lead to a poorer prognosis by upstaging the occult cancer. A strategy to optimise women's safety is to morcellate the specimens inside a bag. In-bag morcellation may avoid the dissemination of tissue fragments.
Objectives: To evaluate the effectiveness and safety of protected in-bag extracorporeal manual morcellation during laparoscopic myomectomy compared to intra-abdominal uncontained power morcellation.
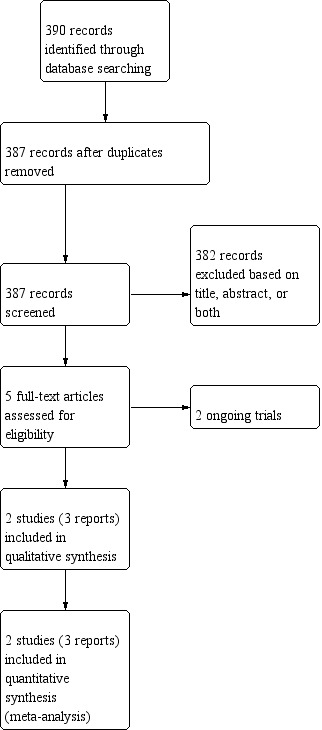
Search methods: On 1 July 2019, we searched; the Cochrane Gynaecology and Fertility Group Specialized Register of Controlled Trials, CENTRAL, MEDLINE, Embase, PsycINFO, CINAHL, LILACS, PubMed, Google Scholar, and two trials registers. We reviewed the reference lists of all retrieved full-text articles, and contacted experts in the field for additional and ongoing trials.
Selection criteria: We included all randomised controlled trials comparing in-bag extracorporeal manual morcellation versus intracorporeal uncontained power morcellation during laparoscopic myomectomy in premenopausal women.
Data collection and analysis: We followed standard Cochrane methods. Two review authors independently reviewed the eligibility of trials, extracted data, and evaluated the risk of bias. Data were checked for accuracy. The summary measures were reported as risk ratios (RR) or mean differences (MD) with 95% confidence interval (CI). The outcomes of interest were a composite of intraoperative and postoperative complications, operative times, ease of morcellation, length of hospital stay, postoperative pain, conversion to laparotomy, and postoperative diagnosis of leiomyosarcoma. Results for the five main outcomes follow.
Main results: We included two trials, enrolling 176 premenopausal women with fibroids, who underwent laparoscopic myomectomy. The experimental group received in-bag manual morcellation, during which each enucleated myoma was placed into a specimen retrieval bag, and manually morcellated with scalpel or scissors. In the control group, intracorporeal uncontained power morcellation was used to reduce the size of the myomas. No intraoperative complications, including accidental morcellation of the liver, conversion to laparotomy, endoscopic bag disruption, bowel injury, bleeding, accidental injury to any viscus or vessel, were reported in either group in either trial. We found very low-quality evidence of inconclusive results for total operative time (MD 9.93 minutes, 95% CI -1.35 to 21.20; 2 studies, 176 participants; I² = 35%), and ease of morcellation (MD -0.73 points, 95% CI -1.64 to 0.18; 1 study, 104 participants). The morcellation operative time was a little longer for the in-bag manual morcellation group, however the quality of the evidence was very low (MD 2.59 minutes, 95% CI 0.45 to 4.72; 2 studies, 176 participants; I² = 0%). There were no postoperative diagnoses of leiomyosarcoma made in either group in either trial. We are very uncertain of any of these results. We downgraded the quality of the evidence due to indirectness and imprecision, because of limited sites in high-income settings and countries, small sample sizes, wide confidence intervals, and few events.
Authors' conclusions: There are limited data on the effectiveness and safety of in-bag morcellation at the time of laparoscopic myomectomy compared to uncontained power morcellation. We were unable to determine the effects of in-bag morcellation on intraoperative complications as no events were reported in either group. We are uncertain if in-bag morcellation improves total operative time or ease of morcellation compared to control. Regarding morcellation operative time, the quality of the evidence was also very low and we cannot be certain of the effect of in-bag morcellation compared to uncontained morcellation. No cases of postoperative diagnosis of leiomyosarcoma occurred in either group. We found only two trials comparing in-bag extracorporeal manual morcellation to intracorporeal uncontained power morcellation at the time of laparoscopic myomectomy. Both trials had morcellation operative time as primary outcome and were not powered for uncommon outcomes such as intraoperative complications, and postoperative diagnosis of leiomyosarcoma. Large, well-planned and executed trials are needed.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
GS reports no conflict of interest.
AR reports no conflict of interest.
FZ and RV are co‐authors of one of the trials included in the full review (Venturella 2016). They were not involved in the assessment of eligibility or risk of bias for this trial. It was assessed by GS and AR.
Figures



















Update of
- doi: 10.1002/14651858.CD013352
Similar articles
-
Can In-Bag Manual Morcellation Represent an Alternative to Uncontained Power Morcellation in Laparoscopic Myomectomy? A Randomized Controlled Trial.Gynecol Obstet Invest. 2018;83(1):52-56. doi: 10.1159/000477171. Epub 2017 Jun 7. Gynecol Obstet Invest. 2018. PMID: 28586771 Clinical Trial.
-
In-Bag Manual Extraction of Excised Myomas by Surgical Scalpel through Suprapubic Mini-Laparotomic Incision in Laparoscopic-Assisted Myomectomy.J Minim Invasive Gynecol. 2016 Jul-Aug;23(5):731-8. doi: 10.1016/j.jmig.2016.02.020. Epub 2016 Mar 3. J Minim Invasive Gynecol. 2016. PMID: 26946277
-
In-bag manual versus uncontained power morcellation for laparoscopic myomectomy: randomized controlled trial.Fertil Steril. 2016 May;105(5):1369-1376. doi: 10.1016/j.fertnstert.2015.12.133. Epub 2016 Jan 19. Fertil Steril. 2016. PMID: 26801067 Clinical Trial.
-
Electric morcellation-related reoperations after laparoscopic myomectomy and nonmyomectomy procedures.J Minim Invasive Gynecol. 2015 Feb;22(2):163-76. doi: 10.1016/j.jmig.2014.09.006. Epub 2014 Sep 11. J Minim Invasive Gynecol. 2015. PMID: 25218993
-
Laparoscopic myomectomy and morcellation: A review of techniques, outcomes, and practice guidelines.Best Pract Res Clin Obstet Gynaecol. 2018 Jan;46:99-112. doi: 10.1016/j.bpobgyn.2017.09.012. Epub 2017 Sep 29. Best Pract Res Clin Obstet Gynaecol. 2018. PMID: 29078975 Review.
Cited by
-
Tips and Details for Successful Robotic Myomectomy: Single-Center Experience with the First 125 Cases.J Clin Med. 2022 Jun 5;11(11):3221. doi: 10.3390/jcm11113221. J Clin Med. 2022. PMID: 35683608 Free PMC article.
-
Myomectomy: Choosing the Surgical Approach - A Systematic Review.Gynecol Minim Invasive Ther. 2024 Jul 18;13(3):146-153. doi: 10.4103/gmit.gmit_152_23. eCollection 2024 Jul-Sep. Gynecol Minim Invasive Ther. 2024. PMID: 39184254 Free PMC article. Review.
-
Uterine artery embolisation versus myomectomy for premenopausal women with uterine fibroids wishing to avoid hysterectomy: the FEMME RCT.Health Technol Assess. 2022 Apr;26(22):1-74. doi: 10.3310/ZDEG6110. Health Technol Assess. 2022. PMID: 35435818 Free PMC article. Clinical Trial.
-
The incidence of unexpected uterine malignancies in hysterectomies carried out for benign indications.J Cancer Res Clin Oncol. 2023 Jul;149(8):4339-4345. doi: 10.1007/s00432-022-04343-0. Epub 2022 Sep 9. J Cancer Res Clin Oncol. 2023. PMID: 36083311 Free PMC article.
-
Clinical and Histopathological Predictors of Recurrence in Uterine Smooth Muscle Tumor of Uncertain Malignant Potential (STUMP): A Multicenter Retrospective Cohort Study of Tertiary Centers.Ann Surg Oncol. 2022 Dec;29(13):8302-8314. doi: 10.1245/s10434-022-12353-y. Epub 2022 Aug 17. Ann Surg Oncol. 2022. PMID: 35976464 Free PMC article.
References
References to studies included in this review
Frascà 2018 {published data only}
-
- Frascà C, Degli Esposti E, Arena A, Tuzzato G, Moro E, Martelli V, et al. Can in-bag manual morcellation represent an alternative to uncontained power morcellation in laparoscopic myomectomy? A randomized controlled trial. Gynecologic and Obstetric Investigation 2018;83(11):52-6. - PubMed
Venturella 2016 {published data only}
-
- Venturella R, Rocca ML, Lico D, La Ferrera N, Cirillo R, Gizzo S, et al. In-bag manual versus uncontained power morcellation for laparoscopic myomectomy: randomized controlled trial. Fertility and Sterility 2016;105(5):1369-76. - PubMed
-
- Venturella R. Intracorporeal versus extracorporeal morcellation with endobag extraction in patients undergoing laparoscopic myomectomy: clinical efficacy and safety outcomes. Preliminary results of a RCT. Journal of Minimally Invasive Gynecology 2014;21(6):S43.
References to ongoing studies
NCT02777203 {published data only}
-
- NCT02777203. Power morcellation systems for laparoscopic hysterectomy and myomectomy [Safety and efficacy of contained electromechanical power morcellation systems for laparoscopic hysterectomy and myomectomy]. clinicaltrials.gov/ct2/show/NCT02777203 (first posted 19 May 2016).
NCT03281460 {published data only}
-
- NCT03281460. Efficacy of In-bag morcellation (FIBROSAC). clinicaltrials.gov/ct2/show/NCT03281460 (first posted 13 September 2017).
Additional references
Baird 2003
-
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. American Journal of Obstetrics and Gynecology 2003;188:100-7. - PubMed
Bhave Chittawar 2014
Covidence [Computer program]
-
- Veritas Health Innovation Covidence. Version accessed 10 April 2019. Melbourne, Australia: Veritas Health Innovation.Available at covidence.org.
Desai 2015
-
- Desai VB, Guo XM, Xu X. Alterations in surgical technique after FDA statement on power morcellation. American Journal of Obstetrics and Gynecology 2015;212:685-7. - PubMed
Divakar 2008
-
- Divakar H. Asymptomatic uterine fibroids. Best Practice & Research Clinical Obstetrics & Gynaecology 2008;22:643-54. - PubMed
Donnez 2015
-
- Donnez J, Hudecek R, Donnez O, Matule D, Arhendt HJ, Zatik J, et al. Efficacy and safety of repeated use of ulipristal acetate in uterine fibroids. Fertility and Sterility 2015;103:519-27. - PubMed
FDA 2020
-
- FDA. UPDATE: The FDA recommends performing contained morcellation in women when laparoscopic power morcellation is appropriate. https://www.fda.gov/medical-devices/safety-communications/update-fda-rec... 2020.
Giarrè 2019
-
- Giarrè G, Franchini M, Castellacci E, Malune ME, Di Spiezio Sardo A, Saccone G, et al. Ulipristal acetate in symptomatic uterine fibroids. A real-world experience in a multicentric Italian study. Gynecological Endocrinology 2019 Aug 8 [Epub ahead of print];36(2):171-4. [DOI: 10.1080/09513590.2019.1648419] - DOI - PubMed
Glaser 2018
-
- Glaser LM, Friedman J, Tsai S, Chaudhari A, Milad M. Laparoscopic myomectomy and morcellation: a review of techniques, outcomes, and practice guidelines. Best Practice & Research: Clinical Obstetrics & Gynaecology 2018;46:99-112. - PubMed
GRADEpro GDT [Computer program]
-
- McMaster University (developed by Evidence Prime) GRADEpro GDT. Version accessed 10 April 2019. Hamilton (ON): McMaster University (developed by Evidence Prime).Available at gradepro.org.
Higgins 2019
-
- Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). The Cochrane Collaboration, 2019. Available from www.training.cochrane.org/handbook.
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Mollo 2018
Munro 2011
-
- Munro MG, Critchley HO, Broder MS, Fraser IS, FIGO Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. International Journal of Gynaecology and Obstetrics 2011;113:3-13. - PubMed
Pavone 2018
-
- Pavone D, Clemenza S, Sorbi F, Fambrini M, Petraglia F. Epidemiology and risk factors of uterine fibroids. Best Practice & Research: Clinical Obstetrics & Gynaecology 2018;46:3-11. - PubMed
Pritts 2015
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Senapati 2015
-
- Senapati S, Tu FF, Magrina JF. Power morcellators: a review of current practice and assessment of risk. American Journal of Obstetrics and Gynecology 2015;212:18-23. - PubMed
Siedhoff 2017
-
- Siedhoff MT, Doll KM, Clarke-Pearson DL, Rutstein SE. Laparoscopic hysterectomy with morcellation vs abdominal hysterectomy for presumed fibroids: an updated decision analysis following the 2014 Food and Drug Administration safety communications. American Journal of Obstetrics and Gynecology 2017;216:259.e1-259.e6. - PMC - PubMed
Wallach 2004
-
- Wallach EE, Vlahos NF. Uterine myomas: an overview of development, clinical features, and management. Obstetrics and Gynecology 2004;104:393-6. - PubMed
Wise 2004
Wright 2015
-
- Wright JD, Tergas AI, Cui R, Burke WM, Hou JY, Ananth CV, et al. Use of electric power morcellation and prevalence of underlying cancer in women who undergo myomectomy. JAMA Oncology 2015;1:69-77. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical