

Three-dimensional simulation analysis of microdissection testicular sperm extraction for patients with non-obstructive azoospermia
- PMID: 32374923
- PMCID: PMC7522677
- DOI: 10.1111/andr.12812
Three-dimensional simulation analysis of microdissection testicular sperm extraction for patients with non-obstructive azoospermia
Abstract
Background: Microdissection testicular sperm extraction (microTESE) is considered the gold standard method of sperm retrieval from patients with non-obstructive azoospermia (NOA). For careful and thorough examination of seminiferous tubules during microTESE, maximizing surface area of the testicles which we are able to search is essential.
Objectives: To develop a systematic procedure for microTESE to maximize surface area and to achieve high sperm retrieval rate (SRR) in microTESE.
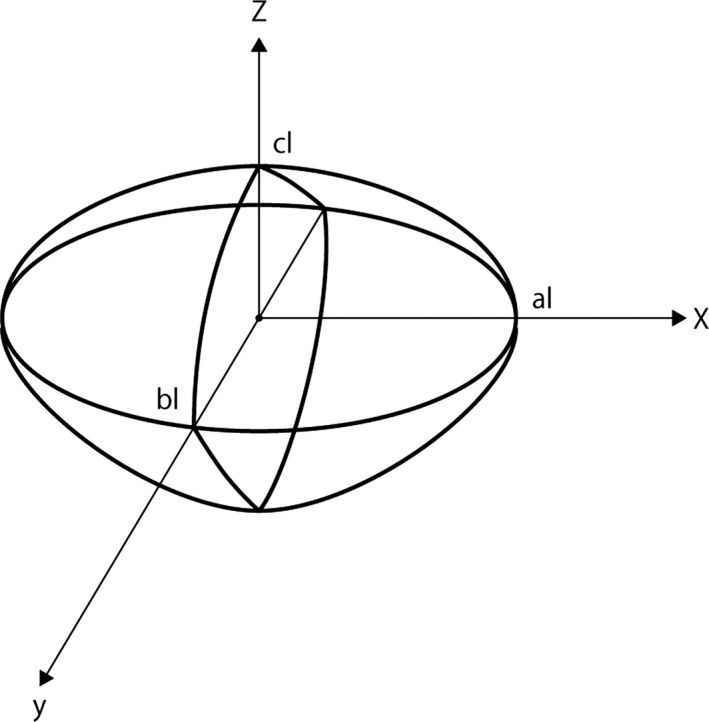
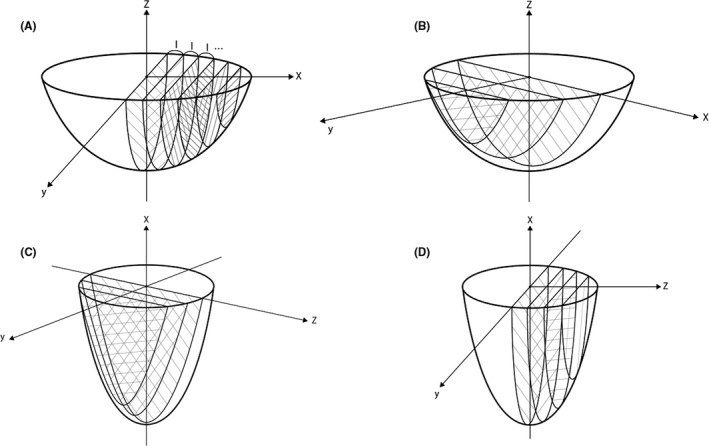
Materials and methods: We simulated microTESE using three-dimensional (3D) simulation model and analyzed mathematically the sum of the surface area in various methods. The best method obtained from this simulation model was applied to 102 patients with NOA from 2014 to 2018. These new clinical results were compared with those of 56 patients who underwent a previous method of microTESE from 2011 to 2014.
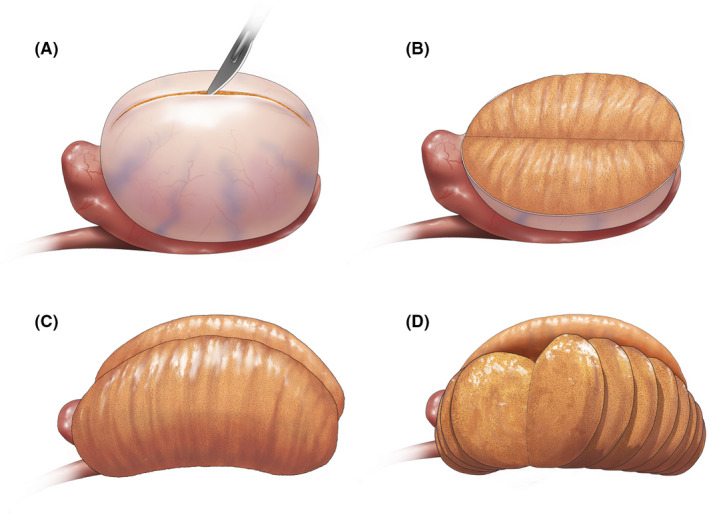
Results: The mathematical 3D simulation model of microTESE indicated that a longitudinal incision on the tunica albuginea and following transverse slicing incisions of testicular parenchyma maximized the surface area coverage. Forty-six (45%) out of 102 patients who underwent microTESE with the new method had successful retrieval of testicular spermatozoa compared with 16 (29%) of 56 patients with the previous method of microTESE (P = .04).
Discussion: Transverse resections of parenchyma in our method run parallel to the courses of intratesticular arteries and do not interfere with the blood supply. The small amount of extracted seminiferous tubules was equivalent to that of the previous method, and no patients exhibited post-operative symptoms of androgen deficiency in our study. As for post-operative pain, our new method was comparable with the previous method. Although our study needs a longer follow-up, there will be limited effects on testicular functions.
Conclusion: Longitudinal incision on the tunica albuginea and following transverse slicing incisions in the testicular parenchyma maximized the surface area and improved the SRR of microTESE.
Keywords: TESE; male infertility; microdissection; non-obstructive azoospermia; simulation; testis.
© 2020 American Society of Andrology and European Academy of Andrology.
Conflict of interest statement
None.
Figures
Similar articles
-
Outcome of microdissection TESE compared with conventional TESE in non-obstructive azoospermia: a systematic review.Andrology. 2014 Jan;2(1):20-4. doi: 10.1111/j.2047-2927.2013.00148.x. Epub 2013 Nov 6. Andrology. 2014. PMID: 24193894
-
Intrasurgical parameters associated with successful sperm retrieval in patients with non-obstructive azoospermia undergoing salvage microdissection testicular sperm extraction.Andrology. 2021 Nov;9(6):1864-1871. doi: 10.1111/andr.13082. Epub 2021 Jul 26. Andrology. 2021. PMID: 34289247
-
The seminiferous tubule caliber pattern as evaluated at high magnification during microdissection testicular sperm extraction predicts sperm retrieval in patients with non-obstructive azoospermia.Andrology. 2019 Jan;7(1):8-14. doi: 10.1111/andr.12548. Epub 2018 Sep 26. Andrology. 2019. PMID: 30259683
-
Mini-incision microdissection testicular sperm extraction: a useful technique for men with cryptozoospermia.Andrology. 2016 Mar;4(2):284-9. doi: 10.1111/andr.12152. Epub 2016 Jan 6. Andrology. 2016. PMID: 26743017
-
Microdissection testicular sperm extraction.Transl Androl Urol. 2017 Aug;6(4):745-752. doi: 10.21037/tau.2017.07.07. Transl Androl Urol. 2017. PMID: 28904907 Free PMC article. Review.
Cited by
-
Micromapping testicular sperm extraction: A new technique for microscopic testicular sperm extraction in nonobstructive azoospermia.Reprod Med Biol. 2024 Mar 11;23(1):e12566. doi: 10.1002/rmb2.12566. eCollection 2024 Jan-Dec. Reprod Med Biol. 2024. PMID: 38476958 Free PMC article.
-
Anatomical considerations, testicular, and scrotal anatomy of nonobstructive azoospermia patients.Asian J Androl. 2025 May 1;27(3):288-292. doi: 10.4103/aja2024102. Epub 2025 Feb 14. Asian J Androl. 2025. PMID: 39949219 Free PMC article. Review.
-
Comparison of unilateral and bilateral microdissection testicular sperm extraction (MD-TESE) in patients with non-obstructive azoospermia: a prospective study.Int Urol Nephrol. 2023 Sep;55(9):2177-2182. doi: 10.1007/s11255-023-03668-0. Epub 2023 Jun 18. Int Urol Nephrol. 2023. PMID: 37330932
-
Use of contrast enhanced ultrasound in testicular diseases: A comprehensive review.Andrology. 2021 Sep;9(5):1369-1382. doi: 10.1111/andr.13057. Epub 2021 Jun 11. Andrology. 2021. PMID: 34043256 Free PMC article. Review.
-
Altered mRNAs Profiles in the Testis of Patients With "Secondary Idiopathic Non-Obstructive Azoospermia".Front Cell Dev Biol. 2022 May 12;10:824596. doi: 10.3389/fcell.2022.824596. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 35646930 Free PMC article.
References
-
- Schlegel PN. Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision. Hum Reprod. 1999;14:131‐135. - PubMed
-
- Friedler S. Outcome of first and repeated testicular sperm extraction and ICSI in patients with non‐obstructive azoospermia. Hum Reprod. 2002;17:2356‐2361. - PubMed
-
- Haimov‐Kochman R, Lossos F, Nefesh I, et al. The value of repeat testicular sperm retrieval in azoospermic men. Fertil Steril. 2009;91:1401‐1403. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
