

Brain responsivity provides an individual readout for motor recovery after stroke
- PMID: 32375172
- PMCID: PMC7296846
- DOI: 10.1093/brain/awaa127
Brain responsivity provides an individual readout for motor recovery after stroke
Abstract
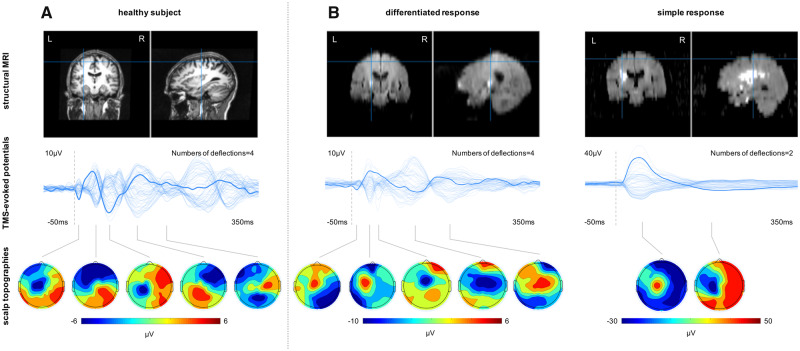
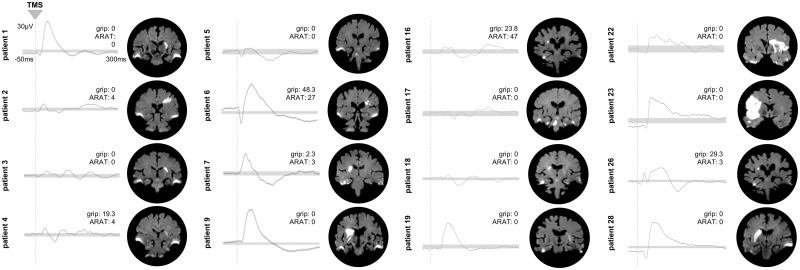
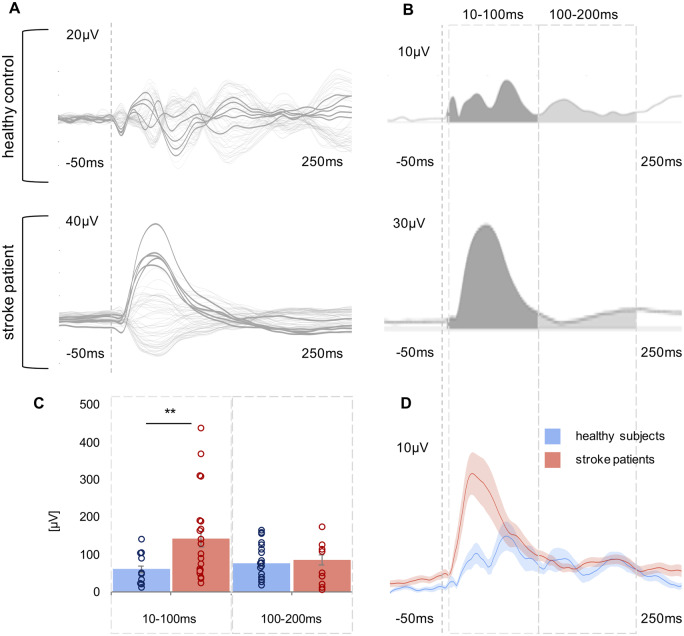
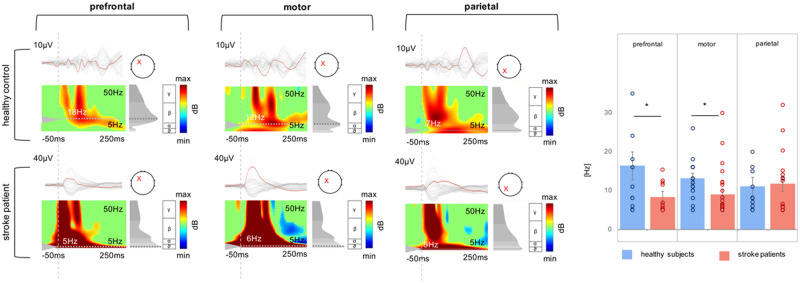
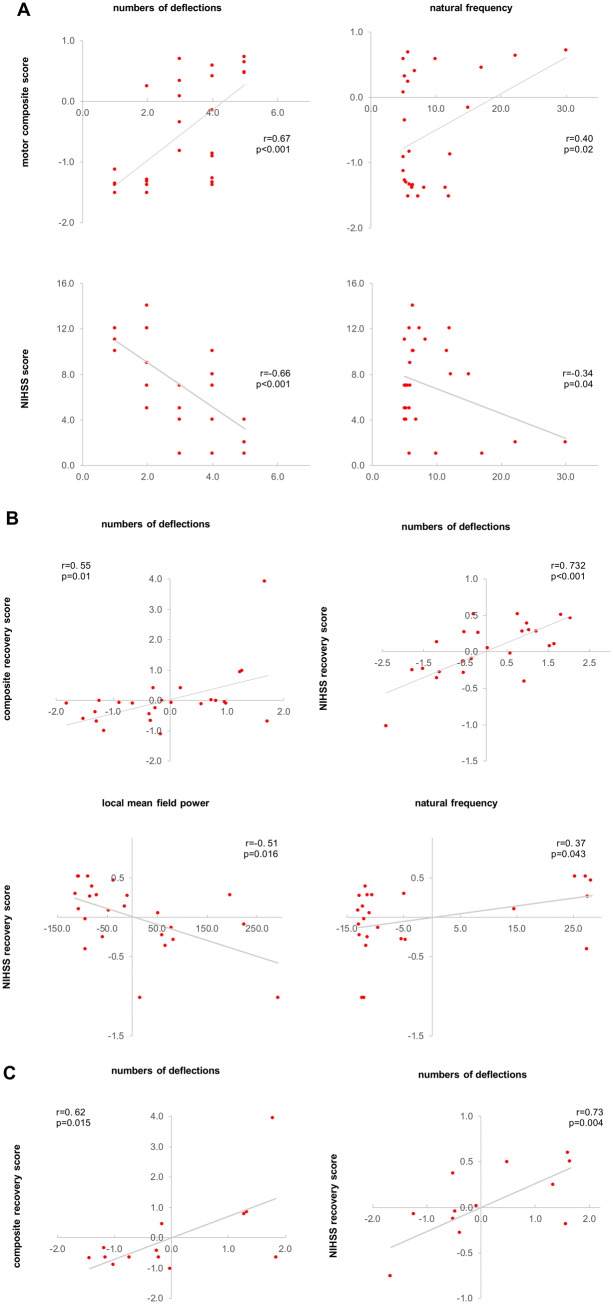
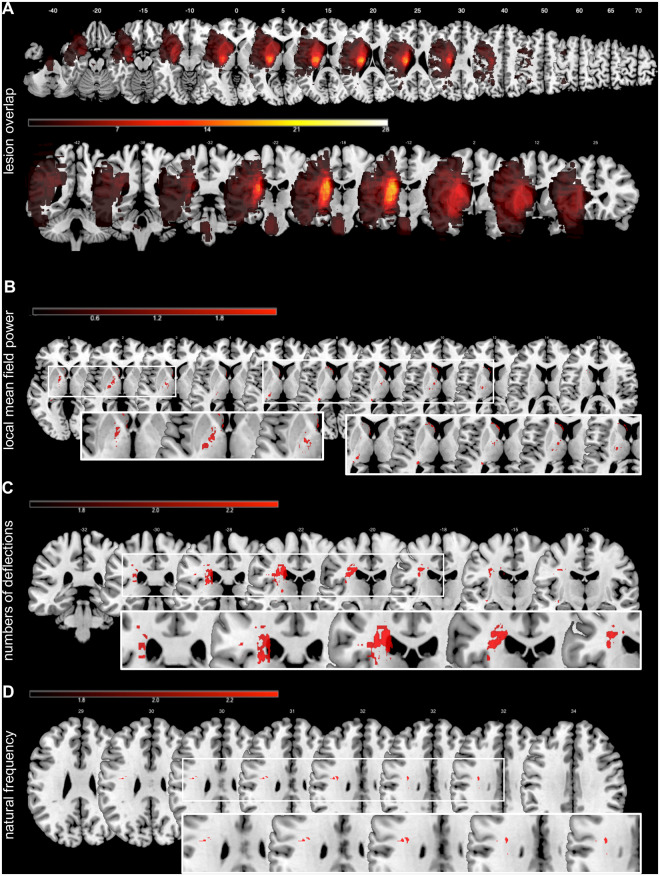
Promoting the recovery of motor function and optimizing rehabilitation strategies for stroke patients is closely associated with the challenge of individual prediction. To date, stroke research has identified critical pathophysiological neural underpinnings at the cellular level as well as with regard to network reorganization. However, in order to generate reliable readouts at the level of individual patients and thereby realize translation from bench to bedside, we are still in a need for innovative methods. The combined use of transcranial magnetic stimulation (TMS) and EEG has proven powerful to record both local and network responses at an individual's level. To elucidate the potential of TMS-EEG to assess motor recovery after stroke, we used neuronavigated TMS-EEG over ipsilesional primary motor cortex (M1) in 28 stroke patients in the first days after stroke. Twenty-five of these patients were reassessed after >3 months post-stroke. In the early post-stroke phase (6.7 ± 2.5 days), the TMS-evoked EEG responses featured two markedly different response morphologies upon TMS to ipsilesional M1. In the first group of patients, TMS elicited a differentiated and sustained EEG response with a series of deflections sequentially involving both hemispheres. This response type resembled the patterns of bilateral activation as observed in the healthy comparison group. By contrast, in a subgroup of severely affected patients, TMS evoked a slow and simplified local response. Quantifying the TMS-EEG responses in the time and time-frequency domain revealed that stroke patients exhibited slower and simple responses with higher amplitudes compared to healthy controls. Importantly, these patterns of activity changes after stroke were not only linked to the initial motor deficit, but also to motor recovery after >3 months post-stroke. Thus, the data revealed a substantial impairment of local effects as well as causal interactions within the motor network early after stroke. Additionally, for severely affected patients with absent motor evoked potentials and identical clinical phenotype, TMS-EEG provided differential response patterns indicative of the individual potential for recovery of function. Thereby, TMS-EEG extends the methodological repertoire in stroke research by allowing the assessment of individual response profiles.
Keywords: TMS-EEG; neurorehabilitation; plasticity; slow waves.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Comment in
-
Structural brain networks and functional motor outcome after stroke-a prospective cohort study.Brain Commun. 2020 Jan 10;2(1):fcaa001. doi: 10.1093/braincomms/fcaa001. eCollection 2020. Brain Commun. 2020. PMID: 32954275 Free PMC article.
-
Connecting to motor recovery after stroke.Brain Commun. 2020 May 6;2(2):fcaa067. doi: 10.1093/braincomms/fcaa067. eCollection 2020. Brain Commun. 2020. PMID: 32954324 Free PMC article.
References
-
- Belardinelli P, Biabani M, Blumberger DM, Bortoletto M, Casarotto S, David O, et al.Reproducibility in TMS-EEG studies: a call for data sharing, standard procedures and effective experimental control. Brain Stimul 2019; 12: 787–90. - PubMed
-
- Bortoletto M, Veniero D, Thut G, Miniussi C.. The contribution of TMS-EEG coregistration in the exploration of the human cortical connectome. Neurosci Biobehav Rev 2015; 49: 114–24. - PubMed
-
- Braack ter EM, de Vos CC, van Putten M.. Masking the auditory evoked potential in TMS-EEG: a comparison of various methods. Brain Topogr 2015; 28: 520–8. - PubMed
