

Genotype characteristics and immunological indicator evaluation of 311 hemophagocytic lymphohistiocytosis cases in China
- PMID: 32375849
- PMCID: PMC7201972
- DOI: 10.1186/s13023-020-01390-z
Genotype characteristics and immunological indicator evaluation of 311 hemophagocytic lymphohistiocytosis cases in China
Abstract
Background: Primary hemophagocytic lymphohistiocytosis (pHLH) is a genetic disorder that is classically diagnosed by genetic testing. Secondary HLH (sHLH) is usually caused by infections, malignancies, or autoimmune disorders, but may display some mutations or polymorphisms. Rapid immunological assays examining natural killer (NK) cell activity, degranulation function (CD107a), and protein expression related to genetic deficiencies have been recommended for early pHLH identification.
Methods: A retrospective analysis of 311 HLH patients from a Chinese population was performed to evaluate the potential correlations between genetic testing and rapid immunological assays; genotyping characteristics, age of onset, and etiology were examined.
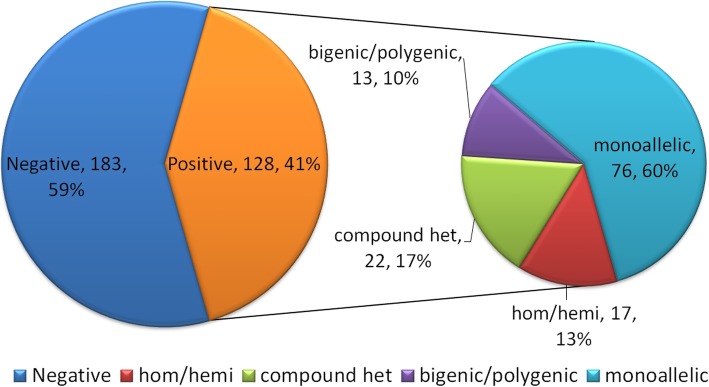
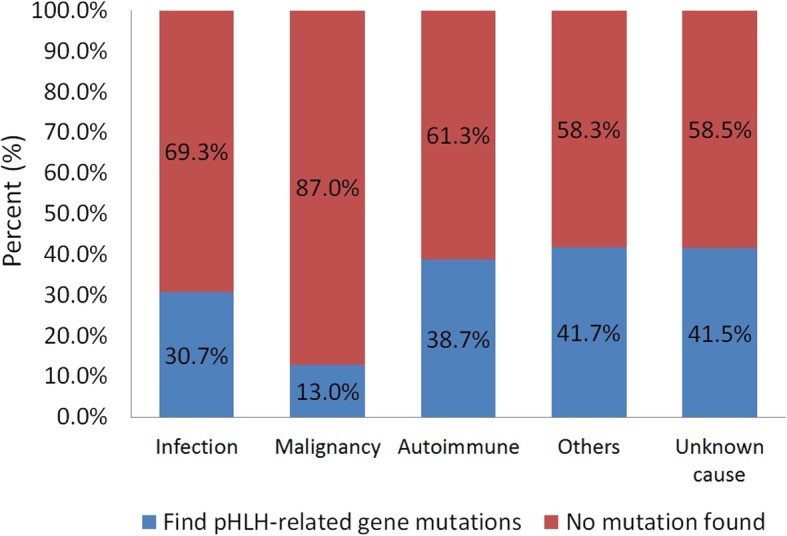
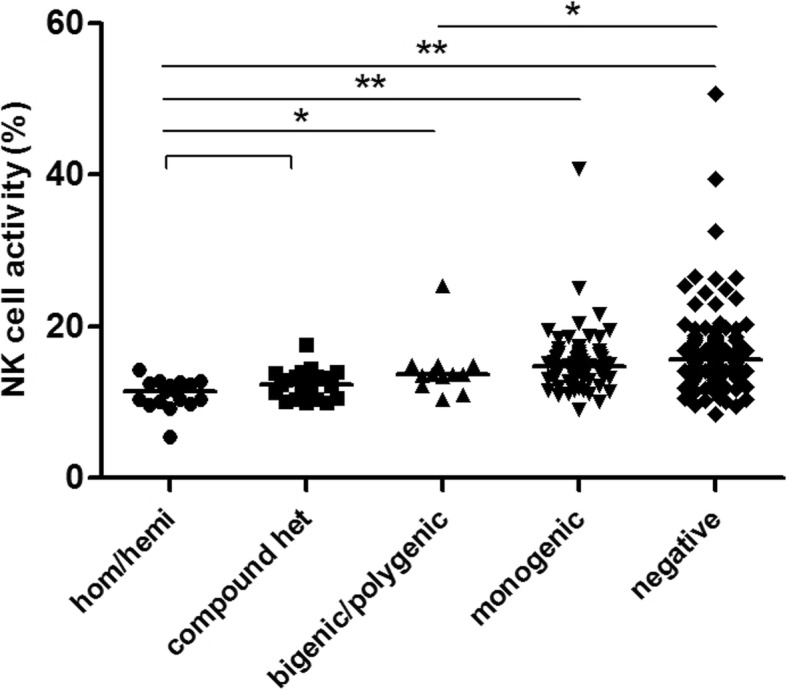
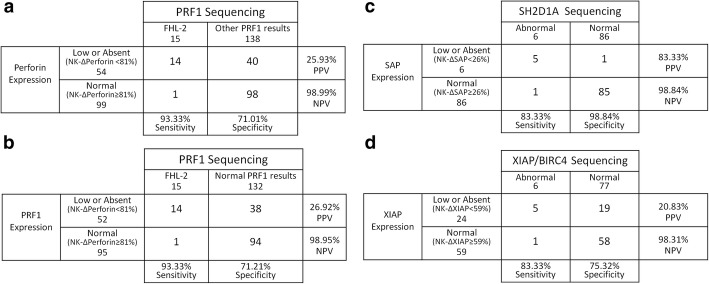
Results: Among the 128 (128/311) patients who were positive in the genetic screening, the most frequently detected mutant gene was UNC13D (29%), followed by LYST (21%), PRF1 (17%), and STXBP2 (10%). Among pHLH patients (n = 39), the majority (67%) had PRF1 and UNC13D defects. FHL-2 was predominant (12/27, 44%) in patients aged under 18, while FHL-3 was the most common (6/12, 50%) in adults. Differences in genetic variant types and etiological components were noted in HLH patients based on the age of onset. NK cell activity and CD107a were observed to show a consistent trend (Ptrend < 0.001) when grouping patients according to the severity of the genetic variant type. Moreover, NK cell activity was generally consistent within a certain range of ΔCD107a values (Ptrend < 0.001). The PPV for bi-allelic degranulation gene mutations in patients with CD107a < 5% was 38.9% (7/18), while the PPV in patients with CD107a ≤10% was 16.7% (13/78). The PPV for pHLH was 41.4% (29/70) with NK cell activity ≤13%. To further evaluate the diagnostic efficacy of NK cell activity assay in pHLH, a receiver operating characteristic (ROC) curve was generated and showed an area under the curve (AUC) of 0.872, and the optimal cutoff value was determined to be 13.425% with a sensitivity of 84.21% and specificity of 80.67% when the corresponding Youden index was maximized. Flow cytometry screening for deficient proteins, including perforin, SAP, and XIAP, showed a relatively high sensitivity (83.33-93.33%). The positive predictive values (PPVs) of perforin and XIAP were relatively low (20.83-26.92%), but the negative predictive values (NPVs) for all three were excellent (all > 98%).
Conclusions: Various immunological indicators have different clinical prediction and application values for the diagnosis of pHLH. The degree of reduction of immunological indicators also needs attention, and choosing appropriate cutoff value may be of important significance in guiding clinical judgment for pHLH.
Keywords: Genetic testing; Primary hemophagocytic lymphohistiocytosis; Rapid immunological indicators.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Chandrakasan S, Filipovich AH. Hemophagocytic lymphohistiocytosis: advances in pathophysiology, diagnosis, and treatment. J Pediatr. 2013;163:1253–1259. - PubMed
-
- Faitelson Y, Grunebaum E. Hemophagocytic lymphohistiocytosis and primary immune deficiency disorders. Clin Immunol. 2014;155:118–125. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
