

A MicroRNA Signature Identifies Pancreatic Ductal Adenocarcinoma Patients at Risk for Lymph Node Metastases
- PMID: 32376411
- PMCID: PMC7483849
- DOI: 10.1053/j.gastro.2020.04.057
A MicroRNA Signature Identifies Pancreatic Ductal Adenocarcinoma Patients at Risk for Lymph Node Metastases
Abstract
Background & aims: Pancreatic ductal adenocarcinomas (PDACs) frequently metastasize to the lymph nodes; strategies are needed to identify patients at highest risk for lymph node metastases. We performed genome-wide expression profile analyses of PDAC specimens, collected during surgery or endoscopic ultrasound-guided fine-need aspiration (EUS-FNA), to identify a microRNA (miRNA) signature associated with metastasis to lymph nodes.
Methods: For biomarker discovery, we analyzed miRNA expression profiles of primary pancreatic tumors from 3 public data sets (The Cancer Genome Atlas, GSE24279, and GSE32688). We then analyzed 157 PDAC specimens (83 from patients with lymph node metastases and 74 without) from Japan, collected from 2001 through 2017, for the training cohort and 107 PDAC specimens (63 from patients with lymph node metastases and 44 without) from a different medical center in Japan, from 2002 through 2016, for the validation cohort. We also analyzed samples collected by EUS-FNA before surgery from 47 patients (22 patients with lymph node metastases and 25 without; 17 for the training cohort and 30 from the validation cohort) and 62 specimens before any treatment from patients who received neoadjuvant chemotherapy (9 patients with lymph node metastasis and 53 without) for additional validation. Multivariate logistic regression analyses were used to evaluate the statistical differences in miRNA expression between patients with vs without metastases.
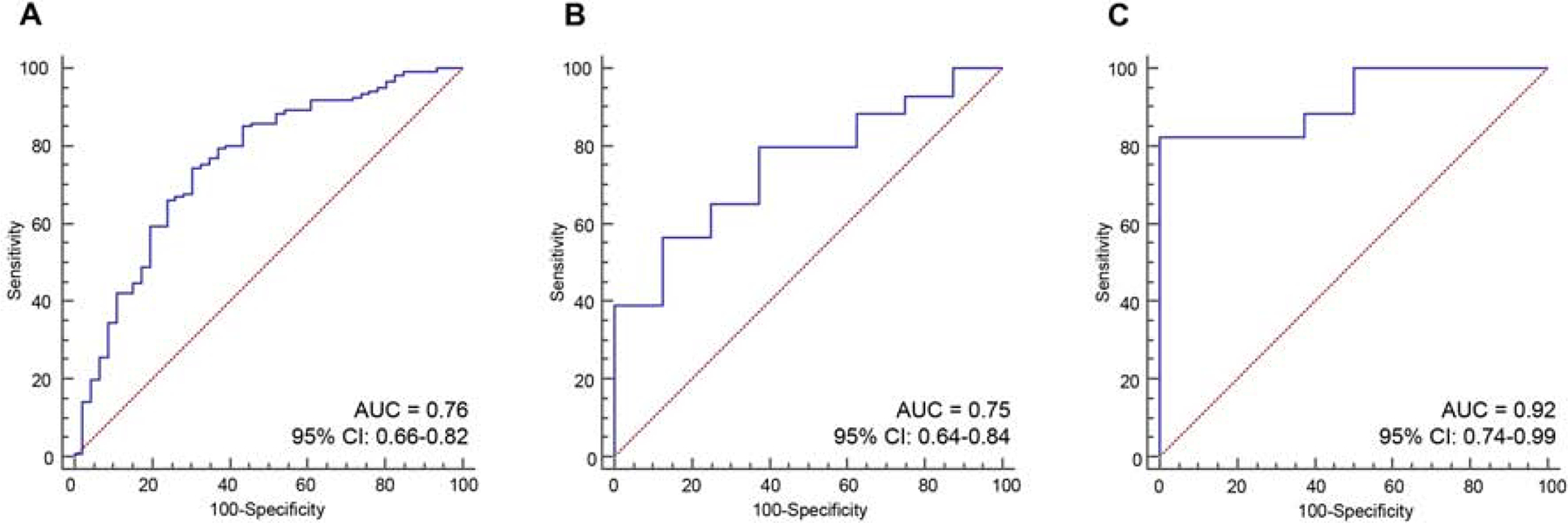
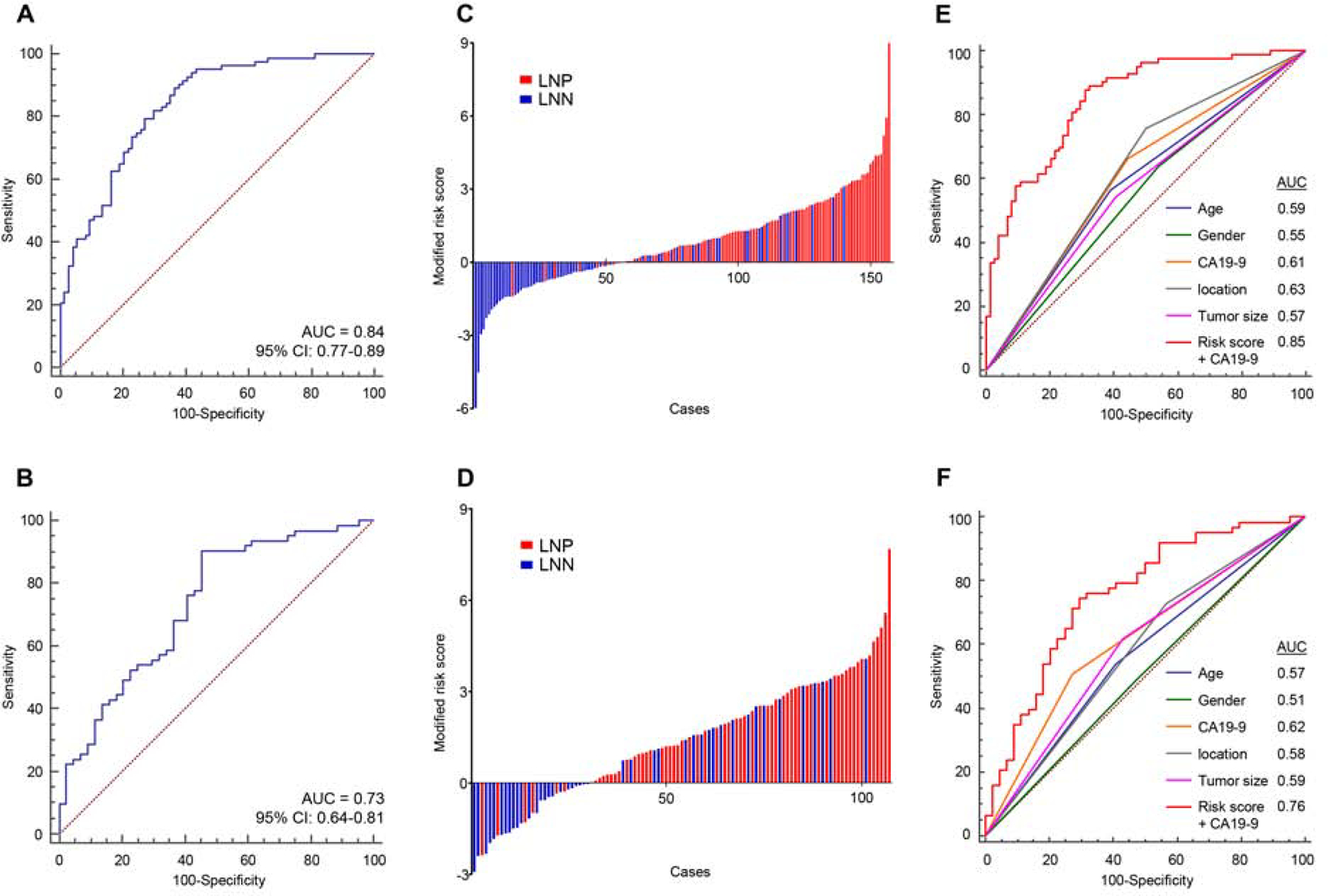
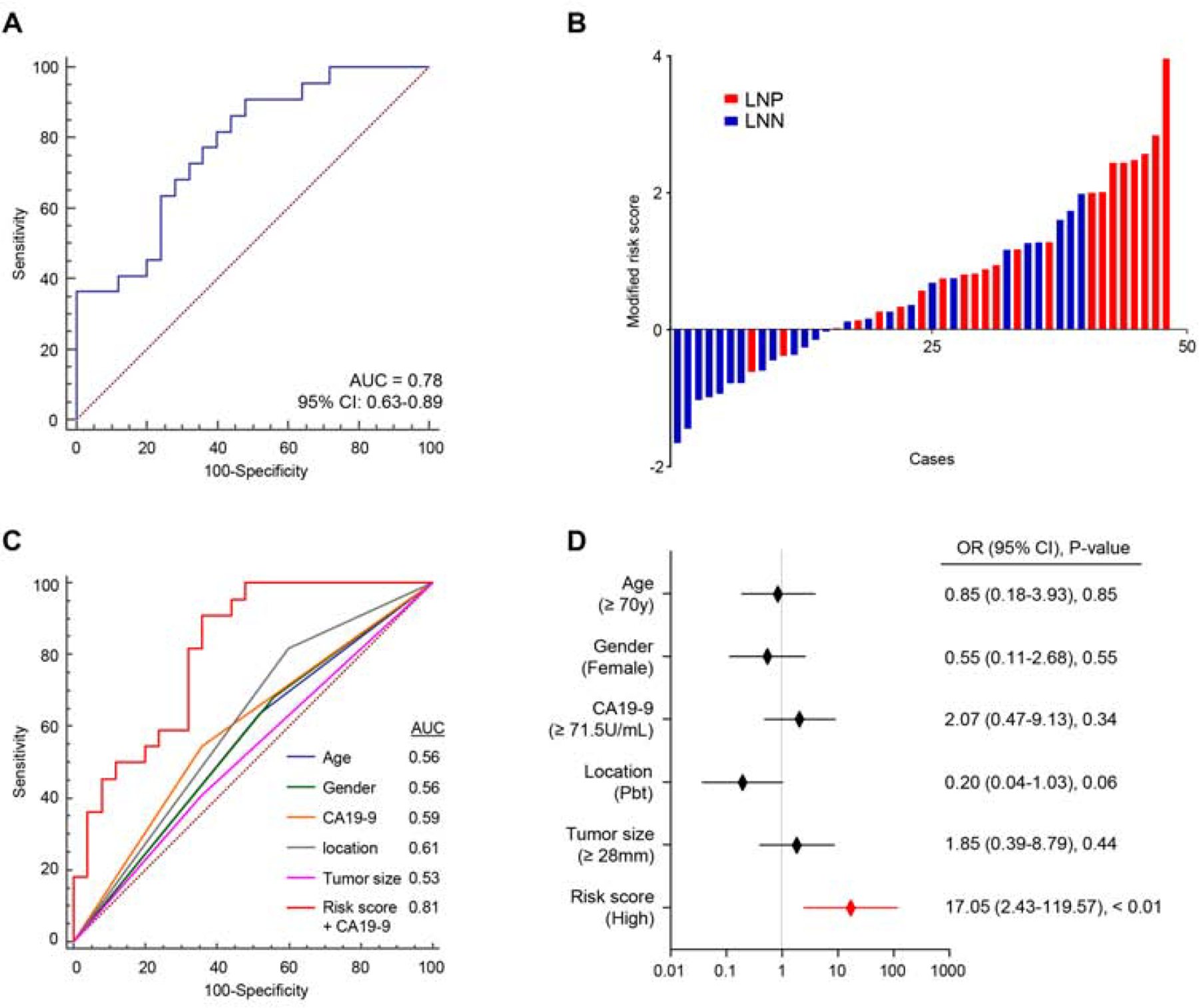
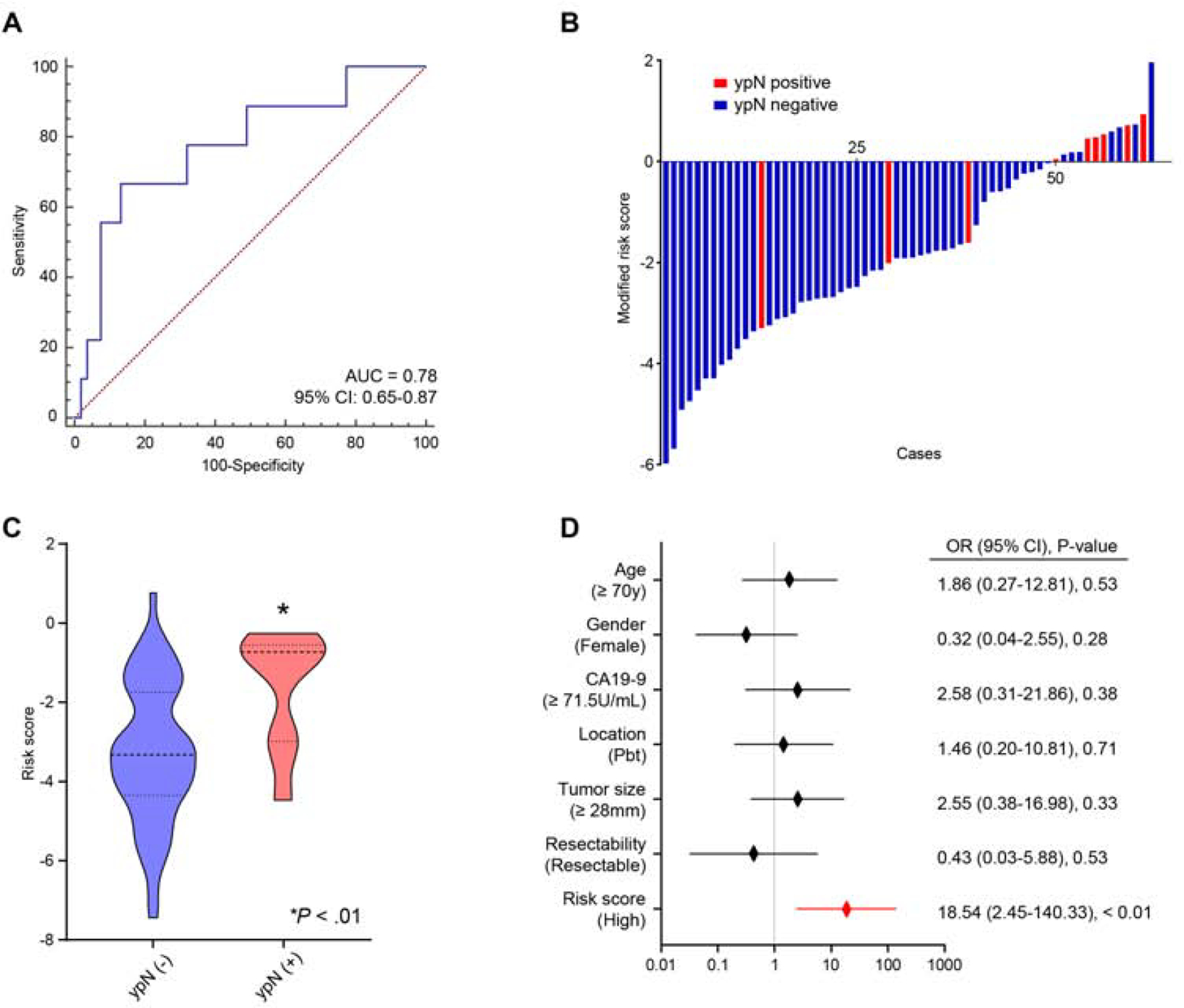
Results: We identified an miRNA expression pattern associated with diagnosis of PDAC metastasis to lymph nodes. Using logistic regression analysis, we optimized and trained a 6-miRNA risk prediction model for the training cohort; this model discriminated patients with vs without lymph node metastases with an area under the curve (AUC) of 0.84 (95% confidence interval [CI], 0.77-0.89). In the validation cohort, the model identified patients with vs without lymph node metastases with an AUC of 0.73 (95% CI, 0.64-0.81). In EUS-FNA biopsy samples, the model identified patients with vs without lymph node metastases with an AUC of 0.78 (95% CI, 0.63-0.89). The miRNA expression pattern was an independent predictor of PDAC metastasis to lymph nodes in the validation cohort (odds ratio, 17.05; 95% CI, 2.43-119.57) and in the EUS-FNA cohort (95% CI, 0.65-0.87).
Conclusions: Using data and tumor samples from 3 independent cohorts, we identified an miRNA signature that identifies patients at risk for PDAC metastasis to lymph nodes. The signature has similar levels of accuracy in the analysis of resected tumor specimens and EUS-FNA biopsy specimens. This model might be used to select treatment and management strategies for patients with PDAC.
Keywords: Cancer Progression; LNM; Prognosis; Prognostic Factor.
Copyright © 2020 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: None of the authors has any potential conflicts to disclose.
Figures
Similar articles
-
Tumor-stroma ratio combined with PD-L1 identifies pancreatic ductal adenocarcinoma patients at risk for lymph node metastases.Br J Cancer. 2025 Jun;132(12):1131-1140. doi: 10.1038/s41416-025-03019-z. Epub 2025 Apr 18. Br J Cancer. 2025. PMID: 40246986 Free PMC article.
-
[Value of endoscopic ultrasound-guided fine needle aspiration in pretest prediction and diagnosis of pancreatic ductal adenocarcinoma].Nan Fang Yi Ke Da Xue Xue Bao. 2018 Sep 30;38(10):1171-1178. doi: 10.3969/j.issn.1673-4254.2018.10.04. Nan Fang Yi Ke Da Xue Xue Bao. 2018. PMID: 30377133 Free PMC article. Chinese.
-
A gene expression signature for predicting response to neoadjuvant chemoradiotherapy in pancreatic ductal adenocarcinoma.Int J Cancer. 2021 Feb 1;148(3):769-779. doi: 10.1002/ijc.33284. Epub 2020 Sep 12. Int J Cancer. 2021. PMID: 32895958 Free PMC article.
-
Needle tract seeding recurrence of pancreatic cancer in the gastric wall with paragastric lymph node metastasis after endoscopic ultrasound-guided fine needle aspiration followed by pancreatectomy: a case report and literature review.BMC Gastroenterol. 2020 Jan 15;20(1):13. doi: 10.1186/s12876-020-1159-x. BMC Gastroenterol. 2020. PMID: 31941458 Free PMC article. Review.
-
Role of endoscopic ultrasound in the molecular diagnosis of pancreatic cancer.World J Gastroenterol. 2014 Aug 21;20(31):10758-68. doi: 10.3748/wjg.v20.i31.10758. World J Gastroenterol. 2014. PMID: 25152579 Free PMC article. Review.
Cited by
-
Deep learning radiomics of dual-energy computed tomography for predicting lymph node metastases of pancreatic ductal adenocarcinoma.Eur J Nucl Med Mol Imaging. 2022 Mar;49(4):1187-1199. doi: 10.1007/s00259-021-05573-z. Epub 2021 Oct 15. Eur J Nucl Med Mol Imaging. 2022. PMID: 34651229
-
Expression of Selected miRNAs in Undifferentiated Carcinoma with Osteoclast-like Giant Cells (UCOGC) of the Pancreas: Comparison with Poorly Differentiated Pancreatic Ductal Adenocarcinoma.Biomedicines. 2024 Apr 26;12(5):962. doi: 10.3390/biomedicines12050962. Biomedicines. 2024. PMID: 38790924 Free PMC article.
-
Circulating small extracellular vesicles microRNAs plus CA-125 for treatment stratification in advanced ovarian cancer.J Transl Med. 2023 Dec 22;21(1):927. doi: 10.1186/s12967-023-04774-4. J Transl Med. 2023. PMID: 38129848 Free PMC article.
-
A Six-microRNA Signature Nomogram for Preoperative Prediction of Tumor Deposits in Colorectal Cancer.Int J Gen Med. 2022 Jan 18;15:675-687. doi: 10.2147/IJGM.S346790. eCollection 2022. Int J Gen Med. 2022. PMID: 35082517 Free PMC article.
-
MiR-10a in Pancreatic Juice as a Biomarker for Invasive Intraductal Papillary Mucinous Neoplasm by miRNA Sequencing.Int J Mol Sci. 2021 Mar 22;22(6):3221. doi: 10.3390/ijms22063221. Int J Mol Sci. 2021. PMID: 33809988 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913–21. - PubMed
-
- Takahashi H, Ohigashi H, Ishikawa O, et al. Perineural invasion and lymph node involvement as indicators of surgical outcome and pattern of recurrence in the setting of preoperative gemcitabine-based chemoradiation therapy for resectable pancreatic cancer. Ann Surg 2012;255:95–102. - PubMed
-
- Masuda T, Dann AM, Elliott IA, et al. A Comprehensive Assessment of Accurate Lymph Node Staging and Preoperative Detection in Resected Pancreatic Cancer. J Gastrointest Surg 2018;22:295–302. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
