

Surgical Treatment of Primary Hyperparathyroidism: Which Therapy to Whom?
- PMID: 32377085
- PMCID: PMC7192265
- DOI: 10.14744/SEMB.2019.56873
Surgical Treatment of Primary Hyperparathyroidism: Which Therapy to Whom?
Abstract
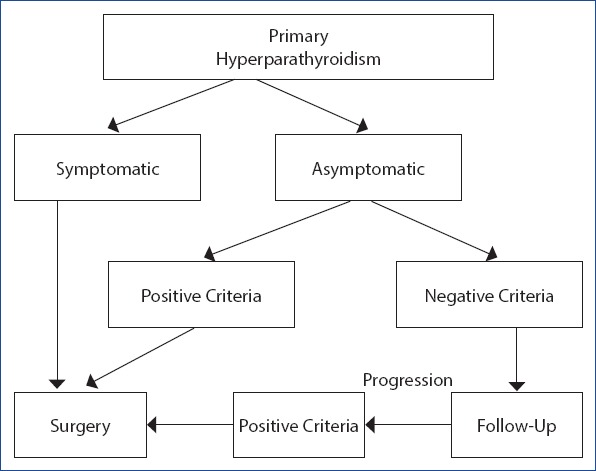
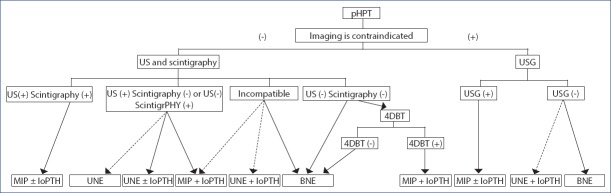
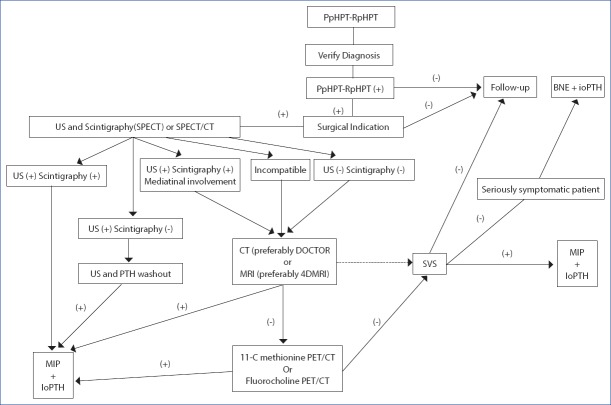
Primary hyperparathyroidism (pHPT) is characterized by an increase in the levels of PTH and Ca, or one of these (Ca, PTH) as a result of a dysregulation of calcium (Ca) metabolism due to inappropriate excess parathyroid hormone (PTH) autonomously produced from one or more than one parathyroid glands. Ninety to 95% of pHPT is a sporadic type, which is not associated with the familial history and other endocrine organ tumors, and 5-10% of it is hereditary. While 80-85% of pHPT arises from a single parathyroid adenoma, 4-5% is caused by a double adenoma, 10-15% by multigland hyperplasia and less than 1% by parathyroid cancer. The diagnosis of pHPT is reached biochemically. The only curative treatment of pHPT is surgery. The choice of surgery in pHPT may vary depending on whether the patient has hereditary HPT or thyroid disease requiring surgical treatment, preoperative localization studies and the findings in these studies, the possibilities of using intraoperative PTH and the preference of the surgeon. The preoperatively determined surgical strategy can be revised according to intraoperative findings in case of need to achieve excellent results. The two main approaches in the surgical treatment of pHPT are BNE (bilateral neck exploration) and MIP (minimal invasive parathyroidectomy). Although BNE is a consistently valid option that has excellent results in the surgical treatment of pHPT and is considered the gold standard, MIP is the ideal approach in selected patients with clinically and radiologically considered a single-gland disease. Negative imaging is not a contraindication for parathyroid surgery and is not a criterion for the presence or absence of surgical indication. Although both methods are safe and effective in the surgical treatment of sporadic pHPT, there is still controversy regarding the effectiveness of both methods. Surgical intervention should establish the risk-benefit balance well, minimize the risk of persistent and recurrent disease and provide the highest cure rate without increasing the risk of complications. Complication rates are higher in the secondary surgery, thus in secondary procedures, selective surgery should be performed under guidance of an imaging modality. The surgical strategy should be determined to achieve maximum cure with minimum dissection and minimal morbidity. In this study, we aimed to determine the type of surgical treatment and pHPT patients suitable for the surgical treatment.
Keywords: Bilateral neck exploration; minimal invasive parathyroidectomy; primary hyperparathyroidism; unilateral neck exploration.
Copyright: © 2019 by The Medical Bulletin of Sisli Etfal Hospital.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Walker MD, Bilezikian JP. Primary hyperparathyroidism:recent advances. Curr Opin Rheumatol. 2018;30:427–39. - PubMed
-
- Uludag M, Aygun N. Primary hyperparathyroidism:Current situation in the clinical and biochemical presentation. Med Bull Sisli Etfal Hosp. 2016;50:171–80.
-
- Mallick R, Chen H. Diagnosis and Management of Hyperparathyroidism. Adv Surg. 2018;52:137–53. - PubMed
Publication types
LinkOut - more resources
Full Text Sources