

Minimally Invasive Open Surgical Approach and Outcomes for Carpal Tunnel Syndrome
- PMID: 32377090
- PMCID: PMC7192267
- DOI: 10.14744/SEMB.2019.94759
Minimally Invasive Open Surgical Approach and Outcomes for Carpal Tunnel Syndrome
Abstract
Objectives: The most common peripheral neuropathy is carpal tunnel syndrome. The present study aims to describe our minimally invasive open surgical approach for carpal tunnel syndrome and evaluate surgical outcomes.
Methods: We included 217 patients who were operated in our clinic for carpal tunnel syndrome by minimally invasive open surgical approach. Visual Analogue Scale and Functional Outcome Scale scores were obtained preoperative, postoperative at one month and three months to determine surgical outcomes.
Results: The mean age of the patients was 55.4±12.8 years (32 to 69), 175 (80.6%) were women and 42 (19.4%) were men. The assessment of carpal tunnel syndrome's etiology showed that 189 (%87.1%) of the cases were idiopathic, 19 (8.8%) had hypothyroidism, 5 (2.3%) had rheumatoid arthritis and 4 (1.8%) were due to pregnancy. The average improvement of VAS between preoperatively and late postoperatively was 5.41±1.05. The average improvement FOS was 17.44±3.06. They were statistically significant.
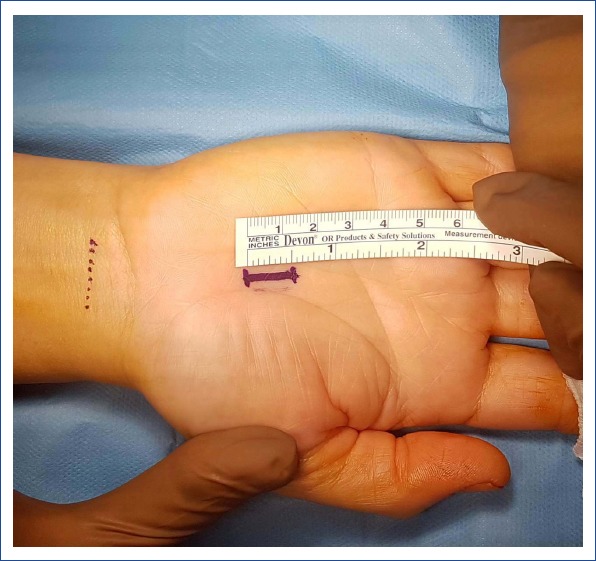
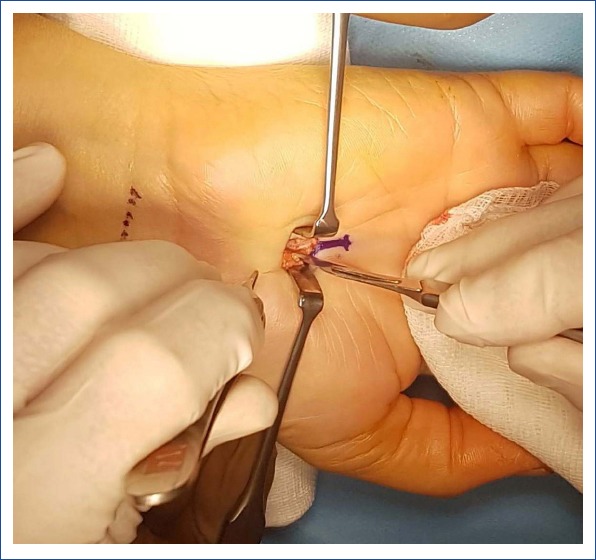
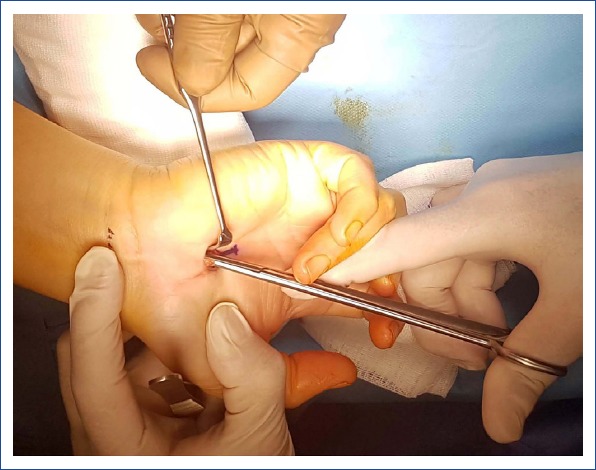
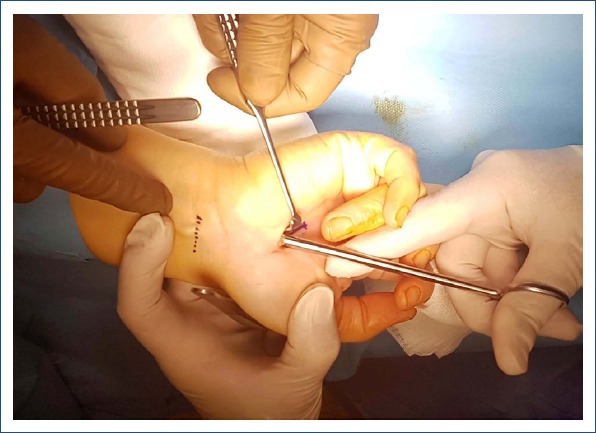
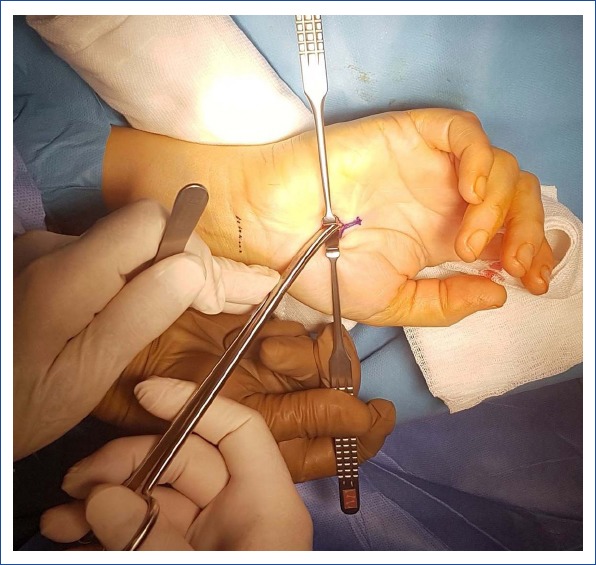
Conclusion: The minimally invasive open surgical approach for carpal tunnel syndrome (an average of 1 cm skin incision) is performed with local anesthesia and successful surgical outcomes are achieved.
Keywords: Carpal tunnel syndrome; minimally invasive open surgical approach; transverse carpal ligament.
Copyright: © 2019 by The Medical Bulletin of Sisli Etfal Hospital.
Conflict of interest statement
Conflict of interest: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this study.
Figures

Similar articles
-
A comparative study on efficacy of modified endoscopic minimally invasive treatment and traditional open surgery for primary carpal tunnel syndrome.J Orthop Surg Res. 2023 Jul 18;18(1):511. doi: 10.1186/s13018-023-03927-x. J Orthop Surg Res. 2023. PMID: 37464402 Free PMC article.
-
The double tunnels technique: an alternative minimally invasive approach for carpal tunnel syndrome.J Neurosurg. 2015 Nov;123(5):1230-7. doi: 10.3171/2014.11.JNS14901. Epub 2015 May 29. J Neurosurg. 2015. PMID: 26024005 Clinical Trial.
-
Minimally invasive carpal tunnel decompression using the KnifeLight.Neurosurgery. 2007 Feb;60(2 Suppl 1):ONS162-8; discussion ONS168-9. doi: 10.1227/01.NEU.0000249249.33052.7E. Neurosurgery. 2007. PMID: 17297379
-
Minimally invasive ultrasound-guided thread carpal tunnel release: a video demonstration protocol.J Ultrasound. 2025 Mar 6. doi: 10.1007/s40477-025-01003-0. Online ahead of print. J Ultrasound. 2025. PMID: 40048109 Review.
-
A comparative meta-analysis between mini-transverse and longitudinal techniques in the management of carpal tunnel syndrome.Surg Neurol Int. 2025 Mar 7;16:78. doi: 10.25259/SNI_520_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 40206736 Free PMC article. Review.
References
-
- Heyman VB. Electrophysiological testing. In: Gelberman RH, editor. Operative nerve repair and reconstruction. 2nd ed. Philadelphia: J.B. Lippincott; 1991. pp. 170–81.
-
- Szabo RM. Entrapment and compression neuropathies. In: Green DP, Hotchkiss RN, Pederson WC, editors. Green's operative hand surgery. 4th ed. Philadelphia: Churchill Livingstone; 1999. pp. 1404–47.
-
- D'Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal tunnel syndrome? JAMA. 2000;283:3110–7. - PubMed
-
- Kerr CD, Gittins ME, Sybert DR. Endoscopic versus open carpal tunnel release:clinical results. Arthroscopy. 1994;10:266–9. - PubMed
-
- Phalen GS. Reflections on 21 years'experience with the carpal-tunnel syndrome. JAMA. 1970;25(212):1365–7. - PubMed
LinkOut - more resources
Full Text Sources