

Requirement of the Preservation of Mental Nerve During the Transfer of Depressor Anguli Oris Composite Flap
- PMID: 32377092
- PMCID: PMC7192271
- DOI: 10.14744/SEMB.2019.04578
Requirement of the Preservation of Mental Nerve During the Transfer of Depressor Anguli Oris Composite Flap
Abstract
Objectives: Reconstruction of wide lower lip defects is still a challenging subject in terms of obtaining functional and aesthetically acceptable results. Lower lip reconstruction with depressor anguli oris muscle was first described by Tobin in 1983. Since the sensory innervation of this composite muscle flap is provided by the mental nerve, it has been advocated that the mental nerve should be preserve during flap elevation. However, no further study has been conducted about this subject since then.
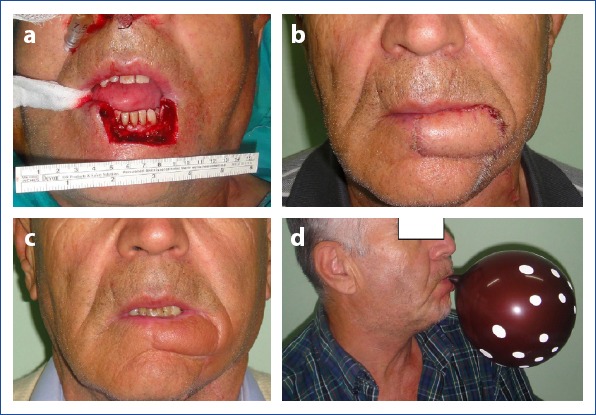
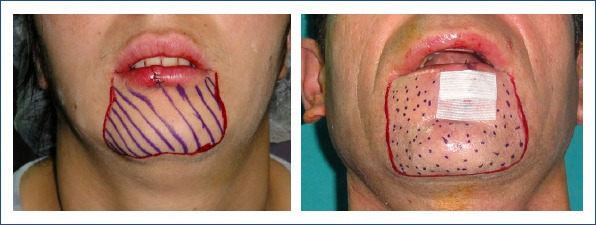
Methods: Sixteen patients with lower lip mass have undergone excisional biopsy. The resultant defects were higher than 30% of the total lower lip. All the defects were reconstructed with Depressor anguli oris composite flaps. In 9 of the patients, the mental nerve was preserved and included to the flap, while in remaining patients it was sacrificed. The results were evaluated in terms of sensation, function, and aesthetic appearance.
Results: In unilaterally reconstructed cases, the results regarding sensation and general complications were similar. However, in bilaterally reconstructed cases, especially where the mental nerve was preserved, the limited arc of rotation has resulted in functional complications, such as whistle deformity in the midline and drooling.
Conclusion: The mental nerve does not just limit the arc of rotation of the Depressör anguli oris composite flap but also remains as a potential route for metastasis via perineural invasion. Preservation and inclusion of the mental nerve during reconstruction with Depressor anguli oris flap do not provide any superior outcome; on the contrary, these results in various unfavorable events make this flap a poor option. The skin and mucosa of the DAO flap are innervated by the buccal branch of the trigeminal nerve; thus, the mental nerve should not be preserved during surgery.
Keywords: Depressor anguli oris; lower lip; mental nerve.
Copyright: © 2019 by The Medical Bulletin of Sisli Etfal Hospital.
Conflict of interest statement
Conflict of interest: None declared.
Figures



Similar articles
-
Functional and Aesthetic Lower Lip Reconstruction With Depressor Anguli Oris Muscle Flap and Reverse Superior Labial Artery Flap.Ann Plast Surg. 2024 Nov 1;93(5):589-596. doi: 10.1097/SAP.0000000000004113. Ann Plast Surg. 2024. PMID: 39445878
-
Lip reconstruction with motor and sensory innervated composite flaps.Clin Plast Surg. 1990 Oct;17(4):623-32. Clin Plast Surg. 1990. PMID: 2249383
-
Combining local flap with depressor anguli oris transfer for lower lip reconstruction and orbicularis oris sphincter function restoration.Clin Oral Investig. 2024 Nov 30;28(12):672. doi: 10.1007/s00784-024-06028-z. Clin Oral Investig. 2024. PMID: 39615004
-
Anatomical Features in Lower-Lip Depressor Muscles for Optimization of Myectomies in Marginal Mandibular Nerve Palsy.J Craniofac Surg. 2021 Sep 1;32(6):2230-2232. doi: 10.1097/SCS.0000000000007622. J Craniofac Surg. 2021. PMID: 33710045 Review.
-
Functional reconstruction of lip defects.Oral Oncol. 2024 Dec;159:107055. doi: 10.1016/j.oraloncology.2024.107055. Epub 2024 Nov 16. Oral Oncol. 2024. PMID: 39551009 Review.
Cited by
-
Complications Following Local-Flap Lip Reconstruction After Tumor Removal: A Systematic Review.Cureus. 2025 May 31;17(5):e85155. doi: 10.7759/cureus.85155. eCollection 2025 May. Cureus. 2025. PMID: 40599512 Free PMC article. Review.
References
-
- Tellioglu AT, Kocer U, Celebioglu S, Sensoz O, Akyuz M. Applications of innervated depressor anguli oris flap in lower lip reconstruction. Türk Plast Cer Derg. 1994;2:41–5.
-
- Siegert R, Weerda H. The history of lip reconstruction. Facial Plast Surg. 1990;7:63–71. - PubMed
-
- Denewer AD, Setit AE, Hussein OA, Aly OF. Functinal and aesthetic outcome of reconstruction of large oro-facial defects involving the lip after tumor resection. J Egypt Natl Canc Inst. 2006;18:61–6. - PubMed
-
- Mazzola RF, Lupo G. Evolving concepts in lip reconstruction. Clin Plast Surg. 1984;11:583–617. - PubMed
-
- Williams EF, 3rd, Setzen G, Mulvaney MJ. Modified Bernard-Burow cheek advancement and cross-lip flap for total lip reconstruction. Arch Otolaryngol Head Neck Surg. 1996;122:1253–8. - PubMed
LinkOut - more resources
Full Text Sources