

Time-critical conditions: assessment of burden and access to care using verbal autopsy in Agincourt, South Africa
- PMID: 32377406
- PMCID: PMC7199706
- DOI: 10.1136/bmjgh-2020-002289
Time-critical conditions: assessment of burden and access to care using verbal autopsy in Agincourt, South Africa
Abstract
Background: Time-critical conditions (TCC) are estimated to cause substantial mortality in low and middle-income countries. However, quantification of deaths and identification of contributing factors to those deaths are challenging in settings with poor health records.
Aim: To use verbal autopsy (VA) data from the Agincourt health and sociodemographic surveillance system in rural South Africa to quantify the burden of deaths from TCC and to evaluate the barriers in seeking, reaching and receiving quality care for TCC leading to death.
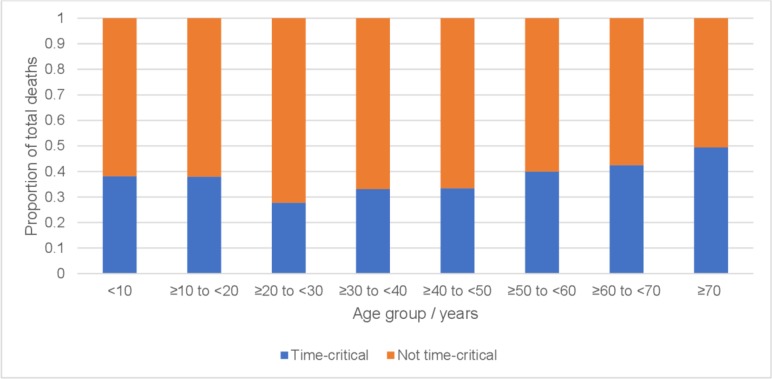
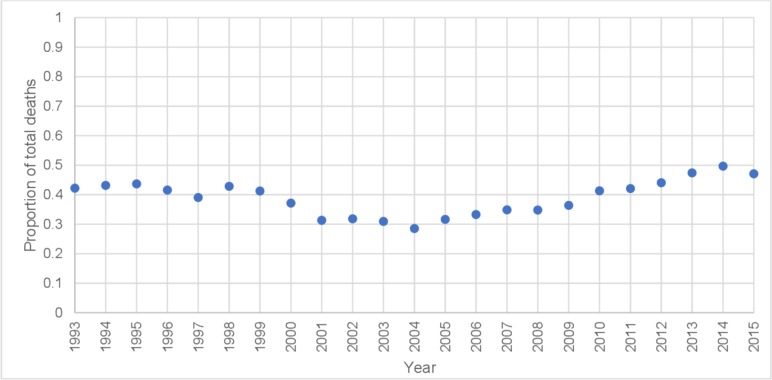
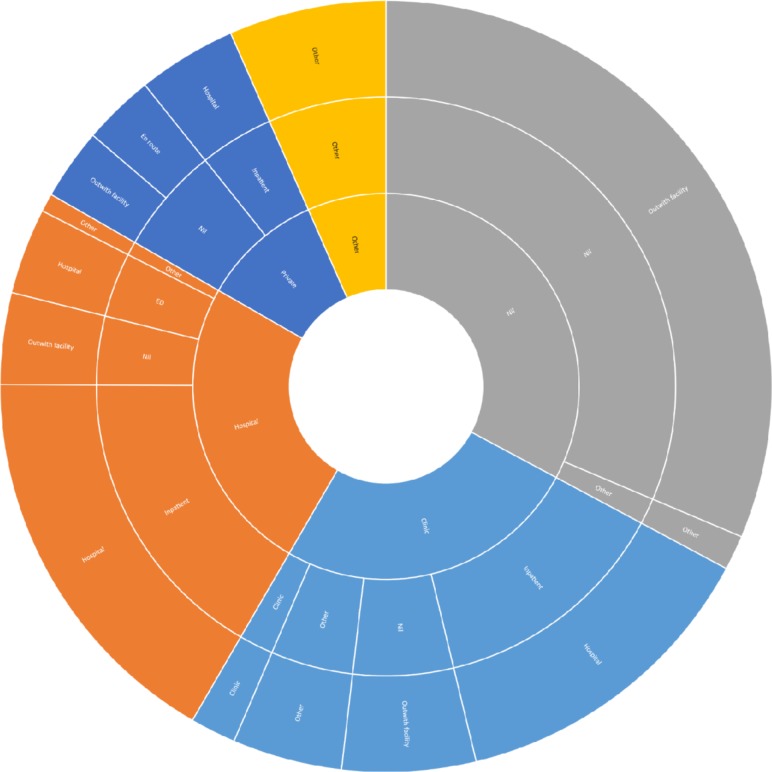
Methodology: Deaths from 1993 to 2015 were analysed to identify causality from TCC. Deaths due to TCC were categorised as communicable, non-communicable, maternal, neonatal or injury-related. Proportion of deaths from TCC by age, sex, condition type and temporal trends was described. Deaths due to TCC from 2012 to 2015 were further examined by circumstances of mortality (CoM) indicators embedded in VA. Healthcare access, at illness onset and during the final day of life, as well as place of death, was extracted from free text summaries. Summaries were also analysed qualitatively using a Three Delays framework to identify barriers to healthcare.
Results: Of 15 305 deaths, 5885 (38.45%) were due to TCC. Non-communicable diseases were the most prevalent cause of death from TCC (2961/5885 cases, 50.31%). CoM indicators highlighted delays in a quarter of deaths due to TCC, most frequently in seeking care. The most common pattern of healthcare access was to die outwith a facility, having sought no healthcare (409/1324 cases, 30.89%). Issues in receipt of quality care were identified by qualitative analysis.
Conclusion: TCCs are responsible for a substantial burden of deaths in this rural South African population. Delays in seeking and receiving quality care were more prominent than those in reaching care, and thus further research and solution development should focus on healthcare-seeking behaviour and quality care provision.
Keywords: health services research; health systems; infections, diseases, disorders, injuries.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Kobusingye OC, Hyder AA, Bishai D, et al. . Emergency medical services. Disease control priorities in developing countries 2006;2:626–8.
-
- Thind A, Hsia R, Mabweijano J, et al. . Prehospital and Emergency Care In: Disease control priorities, third edition (volume 1): essential surgery, 2015: 245–62.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical