

Protected risk stratification with the wearable cardioverter-defibrillator: results from the WEARIT-II-EUROPE registry
- PMID: 32377784
- PMCID: PMC7806570
- DOI: 10.1007/s00392-020-01657-2
Protected risk stratification with the wearable cardioverter-defibrillator: results from the WEARIT-II-EUROPE registry
Erratum in
-
Correction to: Protected risk stratification with the wearable cardioverter-defibrillator: results from the WEARIT-II-EUROPE registry.Clin Res Cardiol. 2021 Jan;110(1):151. doi: 10.1007/s00392-020-01677-y. Clin Res Cardiol. 2021. PMID: 32583061 Free PMC article. No abstract available.
Abstract
Background: The prospective WEARIT-II-EUROPE registry aimed to assess the value of the wearable cardioverter-defibrillator (WCD) prior to potential ICD implantation in patients with heart failure and reduced ejection fraction considered at risk of sudden arrhythmic death.
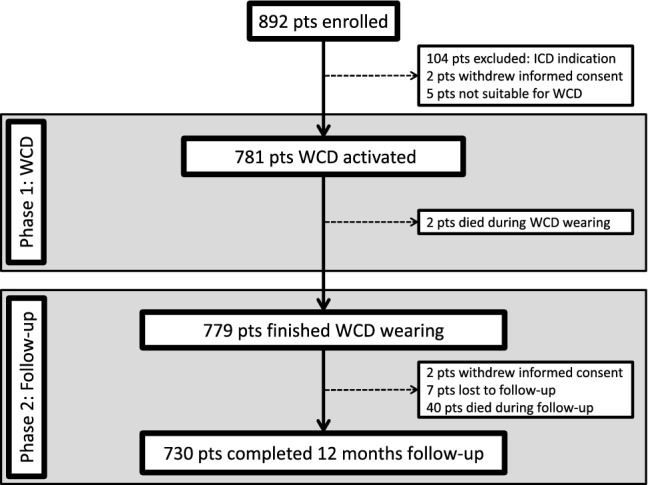
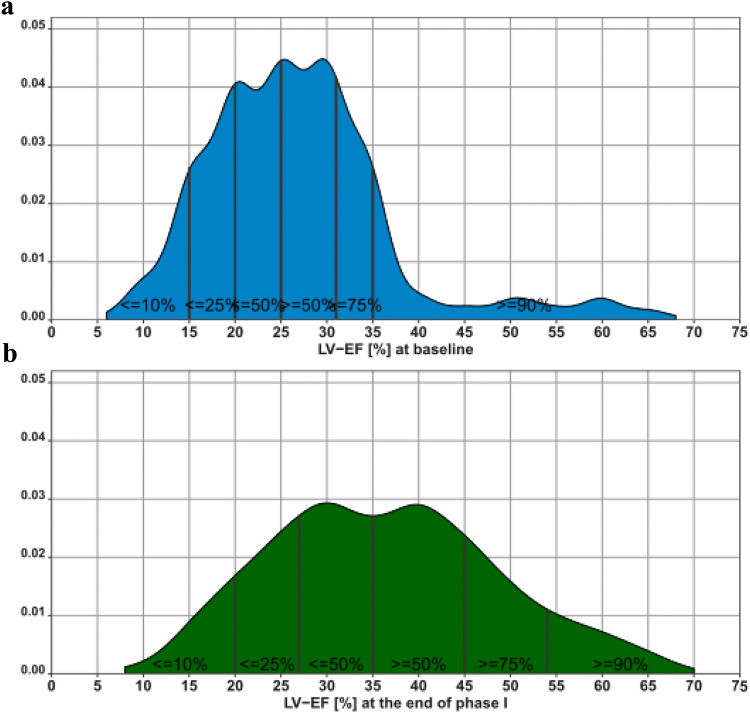
Methods and results: 781 patients (77% men; mean age 59.3 ± 13.4 years) with heart failure and reduced left ventricular ejection fraction (LVEF) were consecutively enrolled. All patients received a WCD. Follow-up time for all patients was 12 months. Mean baseline LVEF was 26.9%. Mean WCD wearing time was 75 ± 47.7 days, mean daily WCD use 20.3 ± 4.6 h. WCD shocks terminated 13 VT/VF events in ten patients (1.3%). Two patients died during WCD prescription of non-arrhythmic cause. Mean LVEF increased from 26.9 to 36.3% at the end of WCD prescription (p < 0.01). After WCD use, ICDs were implanted in only 289 patients (37%). Forty patients (5.1%) died during follow-up. Five patients (1.7%) died with ICDs implanted, 33 patients (7%) had no ICD (no information on ICD in two patients). The majority of patients (75%) with the follow-up of 12 months after WCD prescription died from heart failure (15 patients) and non-cardiac death (15 patients). Only three patients (7%) died suddenly. In seven patients, the cause of death remained unknown.
Conclusions: Mortality after WCD prescription was mainly driven by heart failure and non-cardiovascular death. In patients with HFrEF and a potential risk of sudden arrhythmic death, WCD protected observation of LVEF progression and appraisal of competing risks of potential non-arrhythmic death may enable improved selection for beneficial ICD implantation.
Keywords: Heart failure; Implantable cardioverter-defibrillator; Sudden cardiac death; Wearable cardioverter-defibrillator.
Conflict of interest statement
D. Duncker received lecture honorary, travel support, and/or a fellowship grant from Biotronik, Boehringer Ingelheim, Boston Scientific, Medtronic, Sorin/LivaNova, St. Jude Medical/Abbott, Zoll. J. W. Erath reports receiving travel support and lecture fees from ZOLL Medical and Servier and is a fellow of the Boston Scientific heart rhythm fellowship program, J. C. Geller is a consultant for St. Jude Medical, Biosense Webster, Boston Scientific, Medtronic, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo and Pfizer, and has received speaker fees from St. Jude Medical, Boston Scientific, Medtronic, Biotronik, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Novartis, Pfizer, Sanofi Aventis and Zoll. O. Göing received lecture honoraria from Zoll. H.U. Klein received research grants, travel support and lecture honoraria from ZOLL-Lifecor Medical Corp. (Pittsburgh, PA, USA); consulting fees and lecture honoraria from Boston Scientific. V. Kutyifa received research grants and consulting fees from ZOLL-Lifecor Medical Corp (Pittsburgh, PA, USA and Boston-scientific, F. M, Malur received lecture fees and travel support from ZOLL CMS-Germany and consulting fees and travel support from Boehringer-Ingelheim Germany, C. Veltmann received received lecture honoraria, travel support, consulting fees and research grant from Biotronik, BMS, Boehringer Ingelheim, Boston Scientific, CVRx, Daiichi Sankyo, Medtronic, St. Jude Medical/Abbott, Zoll. N. K. Wäßnig received lecture honoraria from Bayer Vital GmbH, Novartis and ZOLL-CMS, Germany, S. Winter received lecture fees from ZOLL-CMS Germany, Medtronic and Biotronik. M. Roser received grants from CRI during the conduct of the study; grants and personal fees from Biotronik, personal fees from Boston Scientific, personal fees from St. Jude Medical/Abbott, personal fees from ZOLL CMS, personal fees from Bayer Healthcare, personal fees and non-financial support from Berlin Chemie, personal fees from Boehringer Ingelheim, personal fees from Medtronic, outside the submitted work. M. Block received lecture honorary and travel support from ZOLL. C. Perings received lecture honorary from ZOLL. The remaining authors did not declare any potential conflict of interests.
Figures

References
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC) Europace. 2015;17:1601–1687. doi: 10.1093/europace/euv319. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
