

Tracheostomy in patients with acute respiratory distress syndrome is not related to quality of life, symptoms of psychiatric disorders or return-to-work: the prospective DACAPO cohort study
- PMID: 32377963
- PMCID: PMC7203349
- DOI: 10.1186/s13613-020-00671-x
Tracheostomy in patients with acute respiratory distress syndrome is not related to quality of life, symptoms of psychiatric disorders or return-to-work: the prospective DACAPO cohort study
Abstract
Background: Acute respiratory distress syndrome (ARDS) is a life-threatening condition that often requires prolonged mechanical ventilation. Tracheostomy is a common procedure with some risks, on the other hand with potential advantages over orotracheal intubation in critically ill patients. This study investigated the association of tracheostomy with health-related quality of life (HRQoL), symptoms of psychiatric disorders and return-to-work of ARDS survivors.
Methods: Data were collected in the context of the prospective observational German-wide DACAPO study. Clinical and demographic patient data and treatment characteristics were obtained from the participating intensive care units (ICU). HRQoL and return-to-work were assessed using patient-reported questionnaires 3, 6 and 12 months after ICU discharge. HRQoL was measured with the Physical and Mental Component Scale of the Short-Form 12 Questionnaire (PCS-12, MCS-12). The prevalence of psychiatric symptoms (depression and post-traumatic stress disorder [PTSD]) was assessed using the Patient Health Questionnaire-9 and the Post-Traumatic Stress Syndrome-14. Physician-diagnosed anxiety and obsessive-compulsive disorder were recorded by patient self-report in the follow-up questionnaires. The associations of tracheostomy with HRQoL, psychiatric symptoms and return-to-work after 12 months were investigated by means of multivariable linear and logistic regression models.
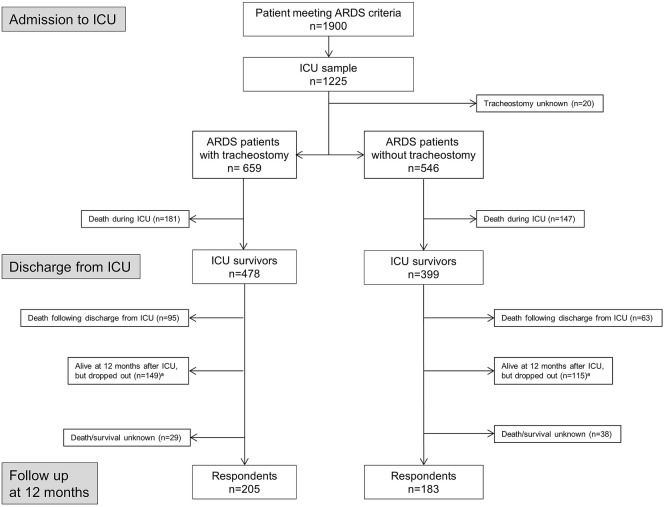
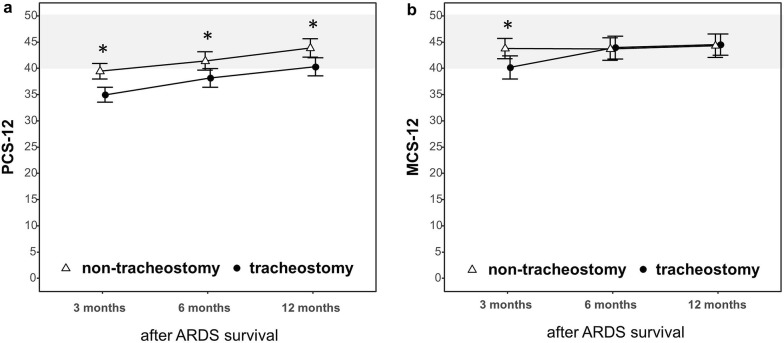
Results: Primary 877 ARDS patients (mean ± standard deviation: 54 ± 16 years, 68% male) survived and were discharged from ICU. Out of these patients, 478 (54.5%) were tracheotomised during ICU treatment. After 12 months, patient-reported outcomes could be analysed of 388 (44.2%) respondents, 205 with tracheostomy and 183 without. One year after ICU discharge, tracheostomy showed no significant association with physical or mental health-related quality of life (PCS-12: - 0.73 [- 3.96, 2.51]; MCS-12: - 0.71 [- 4.92, 3.49]), symptoms of psychiatric disorders (depression: 0.10 [- 1.43, 1.64]; PTSD: 3.31 [- 1.81, 8.43]; anxiety: 1.26 [0.41, 3.86]; obsessive-compulsive disorder: 0.59 [0.05, 6.68]) or return-to-work (0.71 [0.31, 1.64]) in the multivariable analysis (OR [95%-CI]).
Conclusions: Up to 1 year after ICU discharge, neither HRQoL nor symptoms of psychiatric disorders nor return-to-work was affected by tracheostomy. Trial registration NCT02637011 (ClinicalTrials.gov, Registered 15 December 2015, retrospectively registered).
Keywords: ARDS; Health-related quality of life; Intensive care; Return-to-work; Tracheostomy.
Conflict of interest statement
CK received travel grants and lecture fees from Maquet, Rastatt, Germany. TB is a member of the German ARDS-Network and received honoraria for lectures and activities as member of the advisory board of Novalung, Heilbronn, Germany. All other authors (SB, MB, FZ, FDS, SuB and CA) declare no conflict of interest.
Figures
References
-
- Sakr Y, Moreira CL, Rhodes A, Ferguson ND, Kleinpell R, Pickkers P, et al. The impact of hospital and ICU organizational factors on outcome in critically ill patients: results from the extended prevalence of infection in intensive care study. Crit Care Med. 2015;43:519–526. doi: 10.1097/CCM.0000000000000754. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
