

Septic-Associated Encephalopathy: a Comprehensive Review
- PMID: 32378026
- PMCID: PMC7283452
- DOI: 10.1007/s13311-020-00862-1
Septic-Associated Encephalopathy: a Comprehensive Review
Abstract
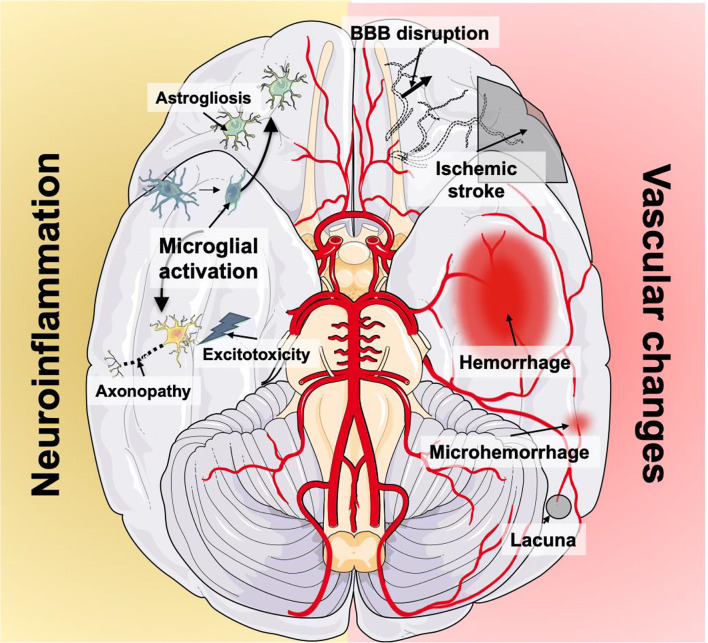
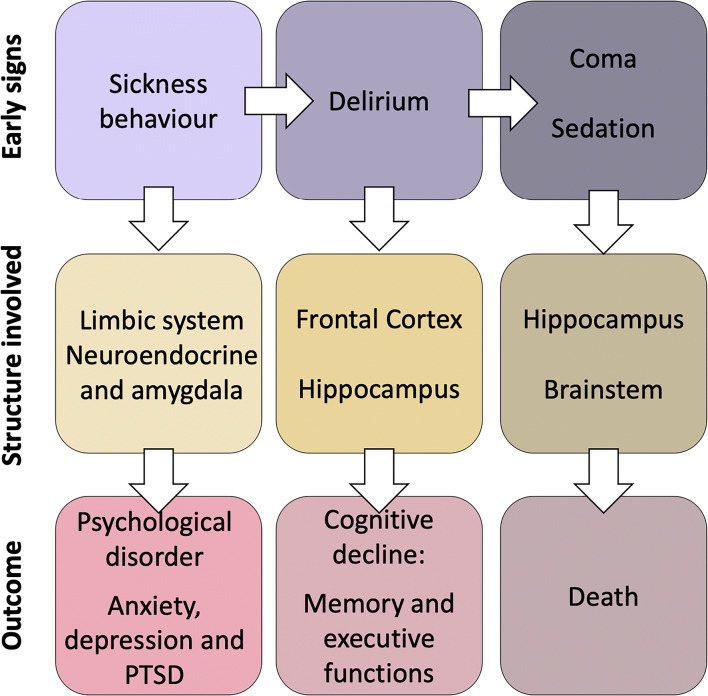
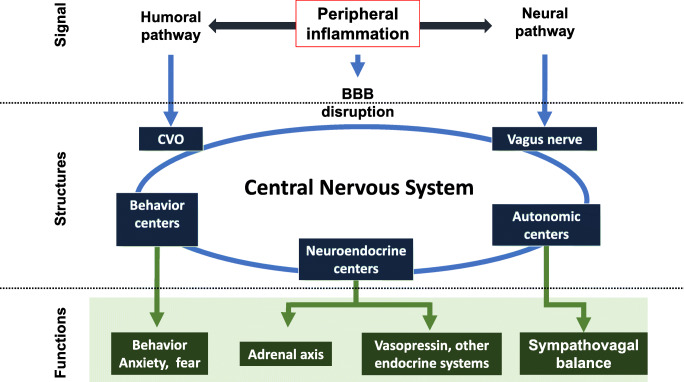
Septic-associated encephalopathy (SAE) is a key manifestation of sepsis, ranging from delirium to coma and occurring in up to 70% of patients admitted to the ICU. SAE is associated with higher ICU and hospital mortality, and also with poorer long-term outcomes, including cognitive and functional outcomes. The pathophysiology of SAE is complex, and it may involve neurotransmitter dysfunction, inflammatory and ischemic lesions to the brain, microglial activation, and blood-brain barrier dysfunction. Delirium (which is included in the SAE spectrum) is mostly diagnosed with validated scales in the ICU population. There is no established treatment for SAE; benzodiazepines should generally be avoided in this setting. Nonpharmacological prevention and management is key for treating SAE; it includes avoiding oversedation (mainly with benzodiazepines), early mobilization, and sleep promotion.
Keywords: Sepsis; blood–brain barrier; microglia; neuroanatomy; neuroinflammation; sepsis-associated encephalopathy.
Figures
References
-
- Mazeraud A, Pascal Q, Verdonk F, Heming N, Chrétien F, Sharshar T. Neuroanatomy and physiology of brain dysfunction in sepsis. Clin Chest Med. 2016;37:333–345. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Eidelman LA, Putterman D, Putterman C, Sprung CL. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA. 1996;275:470–473. - PubMed
-
- Young GB, Bolton CF, Austin TW, Archibald YM, Gonder J, Wells GA. The encephalopathy associated with septic illness. Clin Investig Med Med Clin Exp. 1990;13:297–304. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
