

COVID-19 - Toward a comprehensive understanding of the disease
- PMID: 32378729
- PMCID: PMC8016030
- DOI: 10.5603/CJ.a2020.0065
COVID-19 - Toward a comprehensive understanding of the disease
Abstract
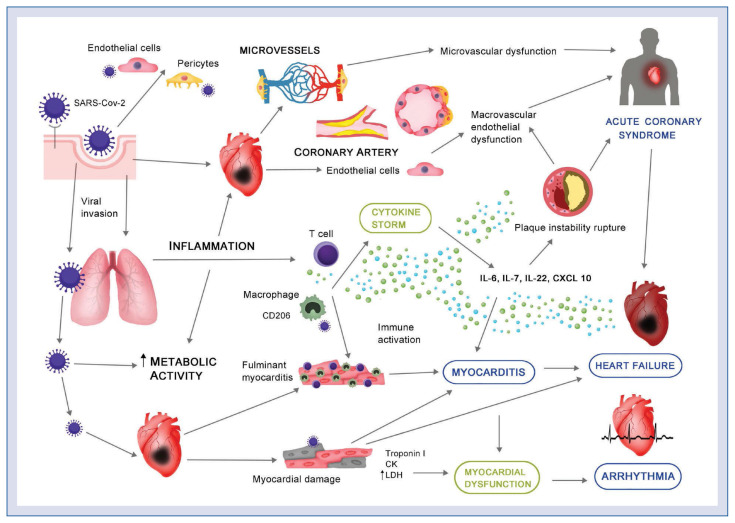
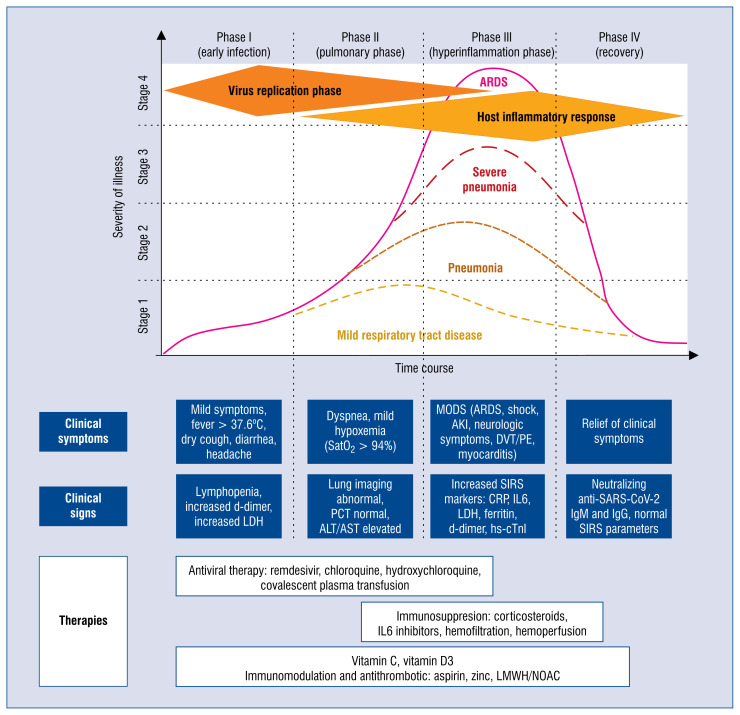
The evidence on the pathophysiology of the novel coronavirus SARS-CoV-2 infection is rapidly growing. Understanding why some patients suffering from COVID-19 are getting so sick, while others are not, has become an informal imperative for researchers and clinicians around the globe. The answer to this question would allow rationalizing the fear surrounding this pandemic. Understanding of the pathophysiology of COVID-19 relies on an understanding of interplaying mechanisms, including SARS-CoV-2 virulence, human immune response, and complex inflammatory reactions with coagulation playing a major role. An interplay with bacterial co-infections, as well as the vascular system and microcirculation affected throughout the body should also be examined. More importantly, a compre-hensive understanding of pathological mechanisms of COVID-19 will increase the efficacy of therapy and decrease mortality. Herewith, presented is the current state of knowledge on COVID-19: beginning from the virus, its transmission, and mechanisms of entry into the human body, through the pathological effects on the cellular level, up to immunological reaction, systemic and organ presentation. Last but not least, currently available and possible future therapeutic and diagnostic options are briefly commented on.
Keywords: COVID-19; SARS-CoV-2; acute respiratory distress syndrome; coagulation; epidemiology; immunology; therapy.
Conflict of interest statement
Figures
References
-
- Smiatacz T. It didn’t have to happen this way – what COVID-19 tells us about translational medicine. Eur J Transl Clin Med. 2020
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
