

Artificial Intelligence and Orthopaedics: An Introduction for Clinicians
- PMID: 32379124
- PMCID: PMC7508289
- DOI: 10.2106/JBJS.19.01128
Artificial Intelligence and Orthopaedics: An Introduction for Clinicians
Abstract
- ➤
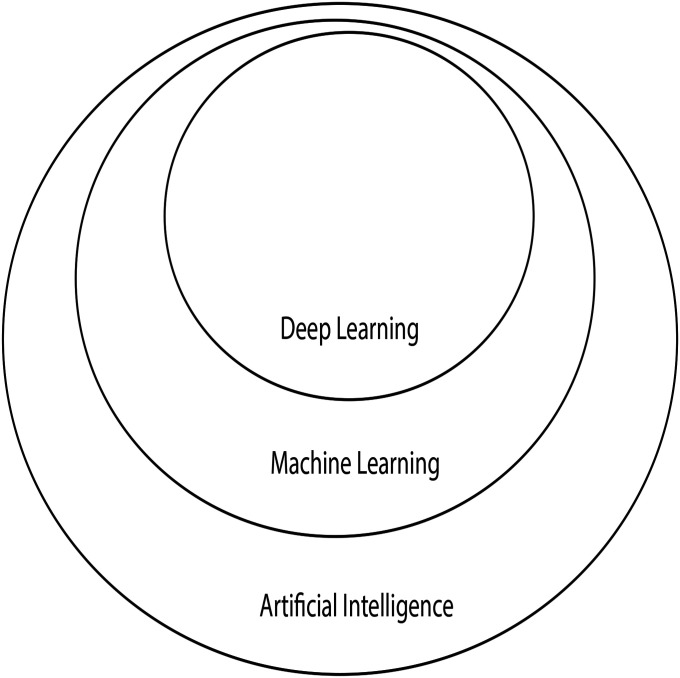
Artificial intelligence (AI) provides machines with the ability to perform tasks using algorithms governed by pattern recognition and self-correction on large amounts of data to narrow options in order to avoid errors.
- ➤
The 4 things necessary for AI in medicine include big data sets, powerful computers, cloud computing, and open source algorithmic development.
- ➤
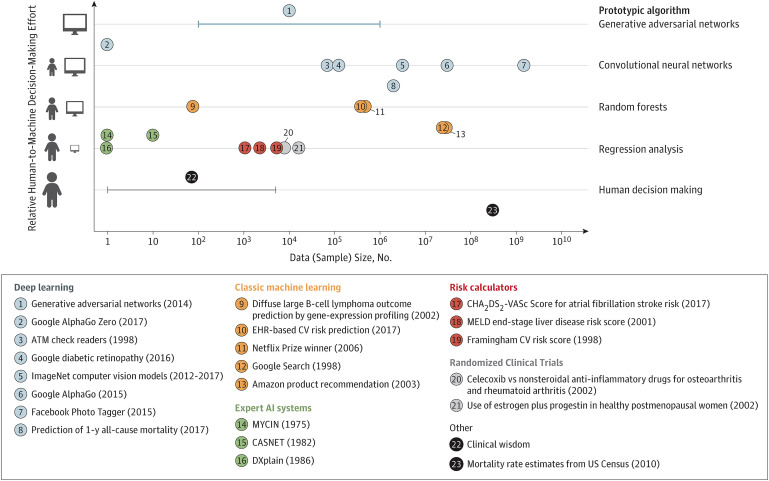
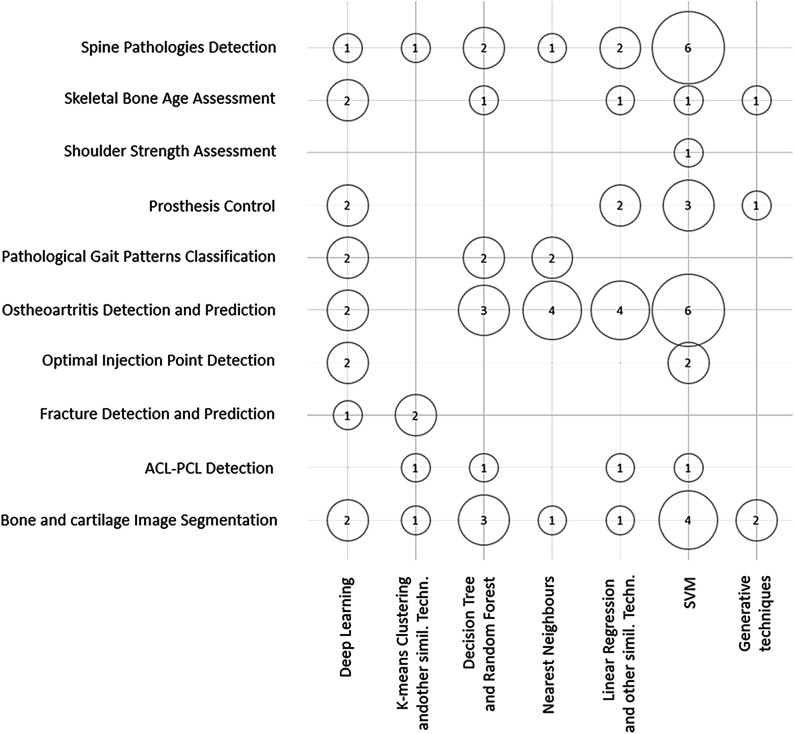
The use of AI in health care continues to expand, and its impact on orthopaedic surgery can already be found in diverse areas such as image recognition, risk prediction, patient-specific payment models, and clinical decision-making.
- ➤
Just as the business of medicine was once considered outside the domain of the orthopaedic surgeon, emerging technologies such as AI warrant ownership, leverage, and application by the orthopaedic surgeon to improve the care that we provide to the patients we serve.
- ➤
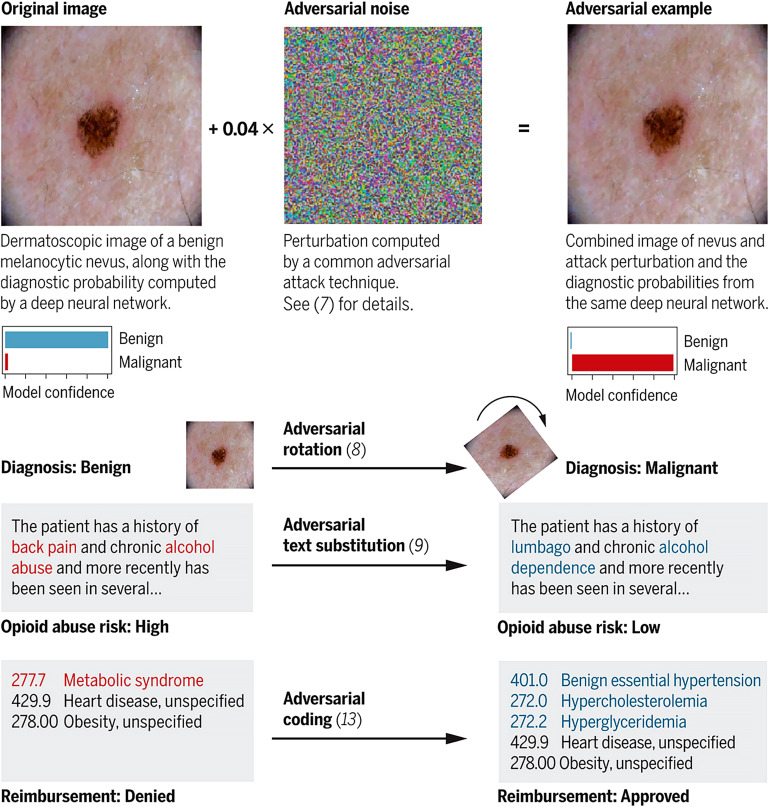
AI could provide solutions to factors contributing to physician burnout and medical mistakes. However, challenges regarding the ethical deployment, regulation, and the clinical superiority of AI over traditional statistics and decision-making remain to be resolved.
Figures


References
-
- Topol EJ. Deep medicine: how artificial intelligence can make healthcare human again. 1st ed. New York: Basic Books; 2019.
-
- Wikipedia. Dartmouth workshop. Accessed 2019 Aug 3. https://en.wikipedia.org/wiki/Dartmouth_workshop
-
- Naylor CD. On the prospects for a (deep) learning health care system. JAMA. 2018. September 18;320(11):1099-100. Epub 2018 Sep 5. - PubMed
-
- Maxmen JS. The post-physician era: medicine in the twenty-first century. New York: Wiley; 1976.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
