

Prevalence of pectus excavatum in an adult population-based cohort estimated from radiographic indices of chest wall shape
- PMID: 32379835
- PMCID: PMC7205298
- DOI: 10.1371/journal.pone.0232575
Prevalence of pectus excavatum in an adult population-based cohort estimated from radiographic indices of chest wall shape
Abstract
Background: Pectus excavatum is the most common chest wall skeletal deformity. Although commonly evaluated in adolescence, its prevalence in adults is unknown.
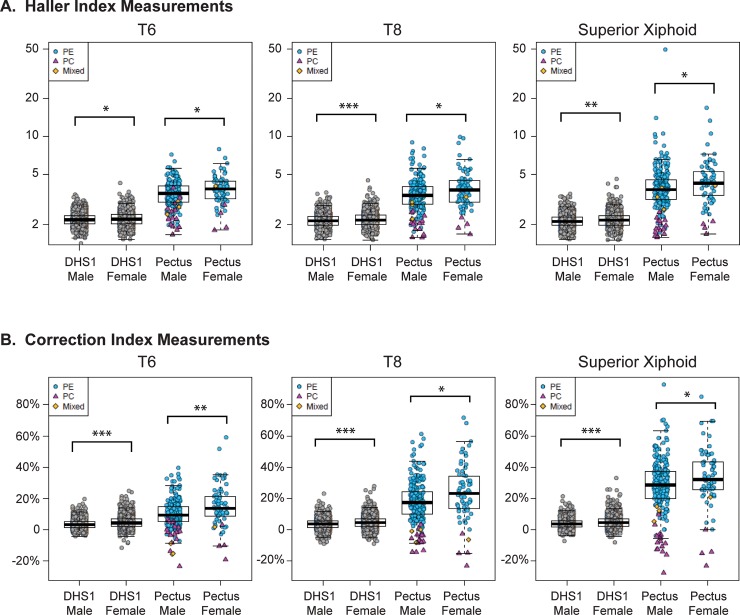
Methods and findings: Radiographic indices of chest wall shape were analyzed for participants of the first (n = 2687) and second (n = 1780) phases of the population-based Dallas Heart Study and compared to clinical cases of pectus (n = 297). Thoracic computed tomography imaging studies were examined to calculate the Haller index, a measure of thoracic axial shape, and the Correction index, which quantitates the posterior displacement of the sternum relative to the ribs. At the level of the superior xiphoid, 0.5%, 5% and 0.4% of adult Dallas Heart Study subjects have evidence of pectus excavatum using thresholds of Haller index >3.25, Correction index >10%, or both, respectively. Radiographic measures of pectus are more common in females than males and there is a greater prevalence of pectus in women than men. In the general population, the Haller and Correction indices are associated with height and weight, independent of age, gender, and ethnicity. Repeat imaging of a subset of subjects (n = 992) demonstrated decreases in the mean Haller and Correction indices over seven years, suggesting change to a more circular axial thorax, with less sternal depression, over time.
Conclusions: To our knowledge, this is the first study estimating the prevalence of pectus in an unselected adult population. Despite the higher reported prevalence of pectus cases in adolescent boys, this study demonstrates a higher prevalence of radiographic indices of pectus in adult females.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Chung CS, Myrianthopoulos NC. Factors affecting risks of congenital malformations. I. Analysis of epidemiologic factors in congenital malformations. Report from the Collaborative Perinatal Project. Birth defects original article series. 1975;11(10):1–22. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
