

Risk Factors for Acute Rejection in the First Year after Lung Transplant. A Multicenter Study
- PMID: 32379979
- PMCID: PMC7427399
- DOI: 10.1164/rccm.201910-1915OC
Risk Factors for Acute Rejection in the First Year after Lung Transplant. A Multicenter Study
Abstract
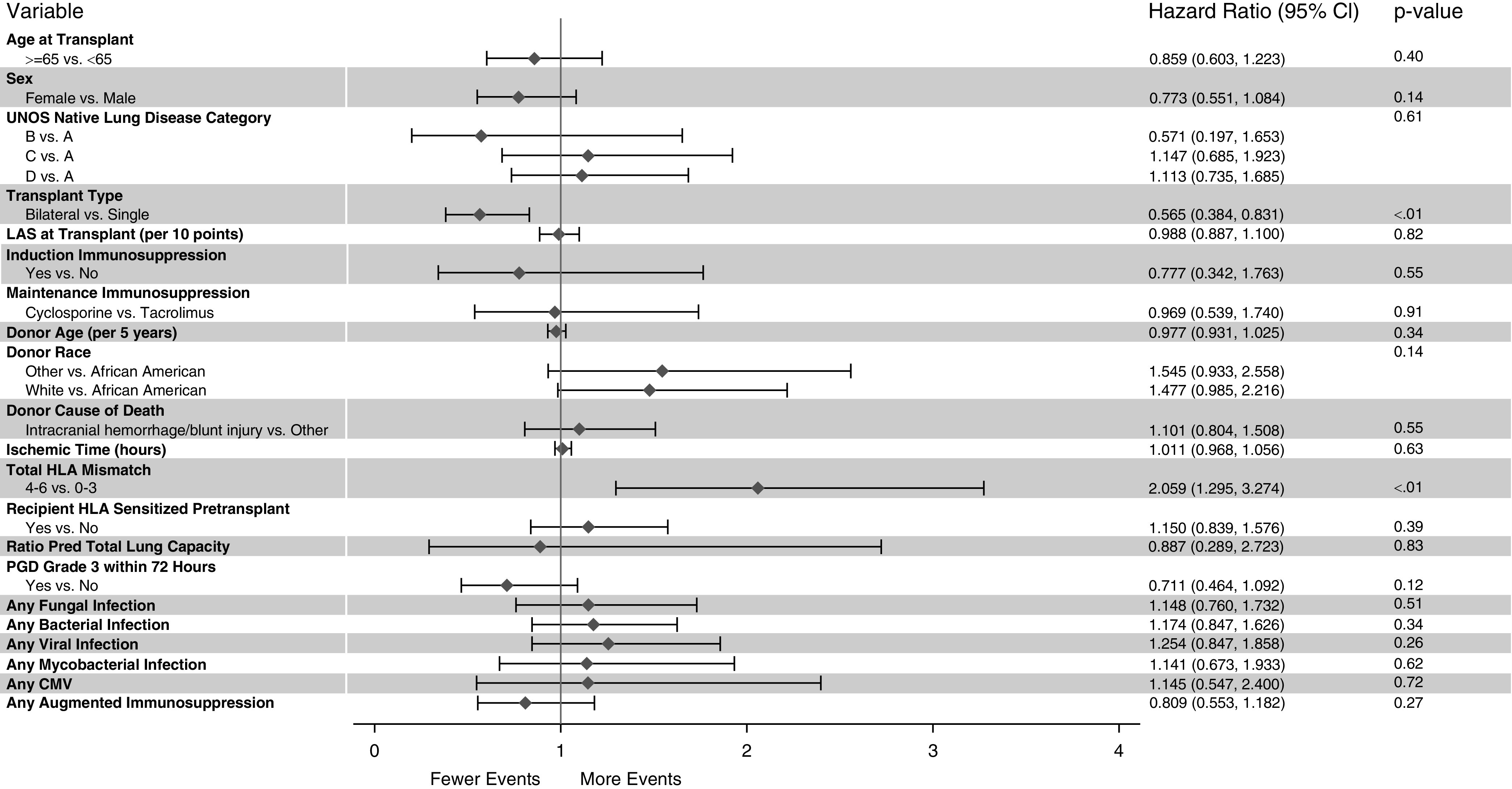
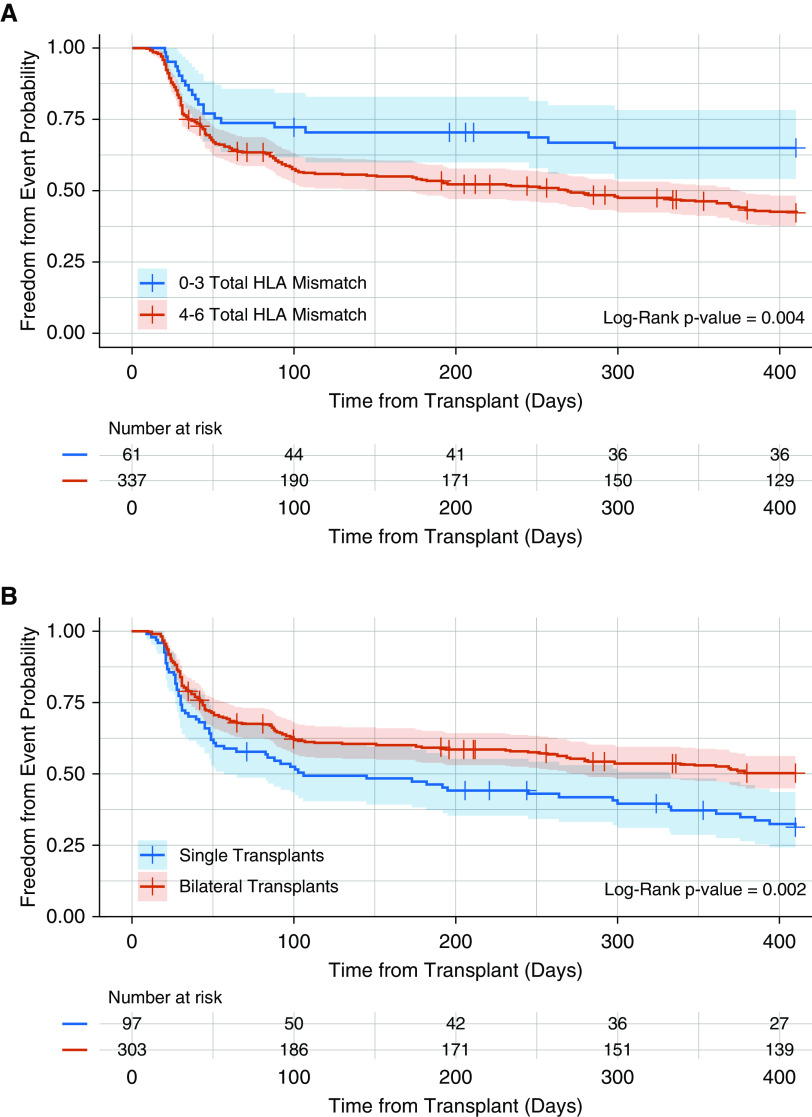
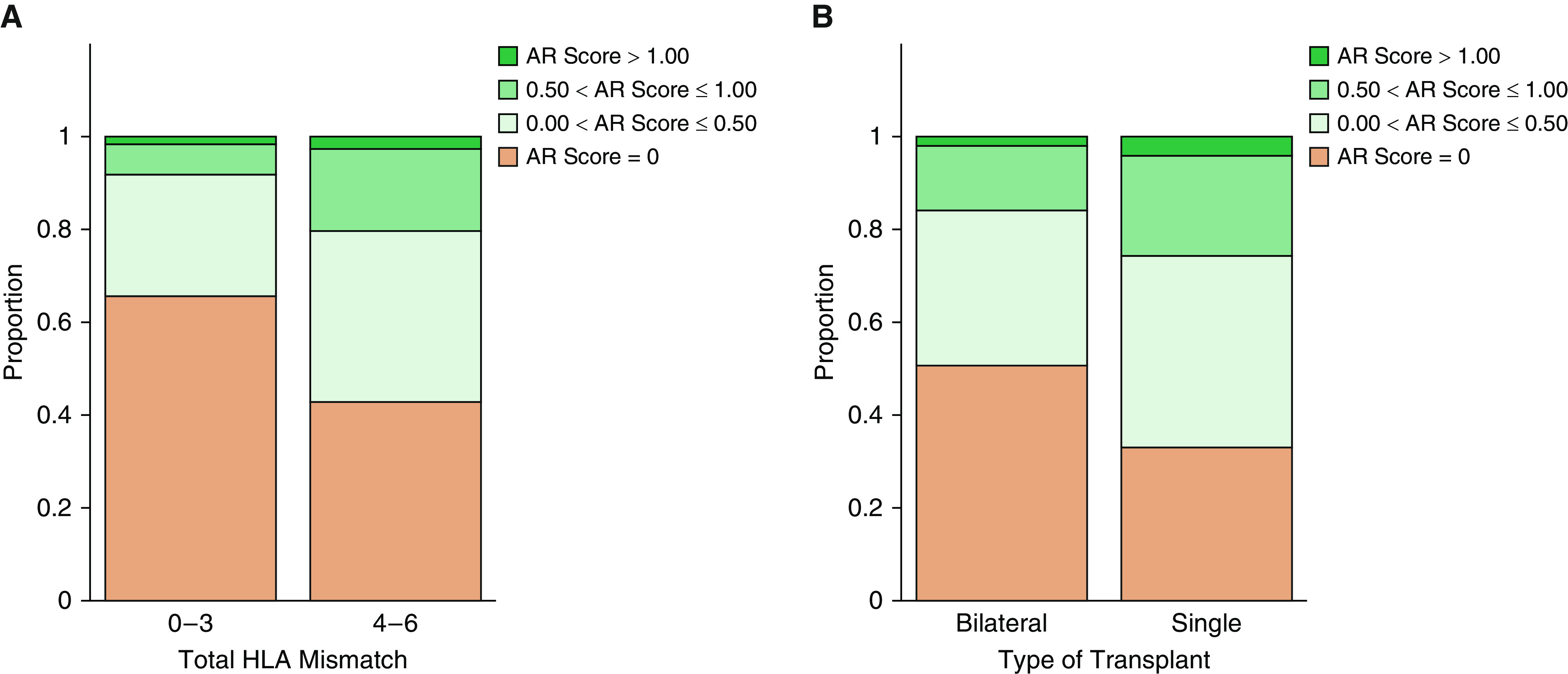
Rationale: Acute rejection, manifesting as lymphocytic inflammation in a perivascular (acute perivascular rejection [AR]) or peribronchiolar (lymphocytic bronchiolitis [LB]) distribution, is common in lung transplant recipients and increases the risk for chronic graft dysfunction.Objectives: To evaluate clinical factors associated with biopsy-proven acute rejection during the first post-transplant year in a present-day, five-center lung transplant cohort.Methods: We analyzed prospective diagnoses of AR and LB from over 2,000 lung biopsies in 400 newly transplanted adult lung recipients. Because LB without simultaneous AR was rare, our analyses focused on risk factors for AR. Multivariable Cox proportional hazards models were used to assess donor and recipient factors associated with the time to the first AR occurrence.Measurements and Main Results: During the first post-transplant year, 53.3% of patients experienced at least one AR episode. Multivariable proportional hazards analyses accounting for enrolling center effects identified four or more HLA mismatches (hazard ratio [HR], 2.06; P ≤ 0.01) as associated with increased AR hazards, whereas bilateral transplantation (HR, 0.57; P ≤ 0.01) was associated with protection from AR. In addition, Wilcoxon rank-sum analyses demonstrated bilateral (vs. single) lung recipients, and those with fewer than four (vs. more than four) HLA mismatches demonstrated reduced AR frequency and/or severity during the first post-transplant year.Conclusions: We found a high incidence of AR in a contemporary multicenter lung transplant cohort undergoing consistent biopsy sampling. Although not previously recognized, the finding of reduced AR in bilateral lung recipients is intriguing, warranting replication and mechanistic exploration.
Keywords: acute rejection; lung transplantation; lymphocytic bronchiolitis.
Figures
Comment in
-
Transforming Diagnostics in Lung Transplantation: From Bronchoscopy to an Artificial Intelligence-driven Approach.Am J Respir Crit Care Med. 2020 Aug 15;202(4):486-488. doi: 10.1164/rccm.202005-1821ED. Am J Respir Crit Care Med. 2020. PMID: 32603183 Free PMC article. No abstract available.
References
-
- Chambers DC, Yusen RD, Cherikh WS, Goldfarb SB, Kucheryavaya AY, Khusch K, et al. International Society for Heart and Lung Transplantation. The registry of the International Society for Heart and Lung Transplantation: thirty-fourth adult lung and heart-lung transplantation report-2017. Focus theme: allograft ischemic time. J Heart Lung Transplant. 2017;36:1047–1059. - PubMed
-
- Khalifah AP, Hachem RR, Chakinala MM, Yusen RD, Aloush A, Patterson GA, et al. Minimal acute rejection after lung transplantation: a risk for bronchiolitis obliterans syndrome. Am J Transplant. 2005;5:2022–2030. - PubMed
-
- Hopkins PM, Aboyoun CL, Chhajed PN, Malouf MA, Plit ML, Rainer SP, et al. Association of minimal rejection in lung transplant recipients with obliterative bronchiolitis. Am J Respir Crit Care Med. 2004;170:1022–1026. - PubMed
-
- Glanville AR, Aboyoun CL, Havryk A, Plit M, Rainer S, Malouf MA. Severity of lymphocytic bronchiolitis predicts long-term outcome after lung transplantation. Am J Respir Crit Care Med. 2008;177:1033–1040. - PubMed
-
- Stewart S, Fishbein MC, Snell GI, Berry GJ, Boehler A, Burke MM, et al. Revision of the 1996 working formulation for the standardization of nomenclature in the diagnosis of lung rejection. J Heart Lung Transplant. 2007;26:1229–1242. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
