

Developing a model for predicting venous thromboembolism in obese pregnant women in a national study
- PMID: 32380308
- PMCID: PMC7298727
- DOI: 10.1016/j.thromres.2020.03.025
Developing a model for predicting venous thromboembolism in obese pregnant women in a national study
Abstract
Introduction: Venous thromboembolism (VTE) in pregnancy and postpartum is a leading cause of maternal morbidity and mortality in developed countries, where obesity is a known risk for this complication. Current guidelines vary in which patients qualify for VTE prophylaxis, precluding a uniform approach for management. We sought to derive a risk prediction model for VTE in obese pregnant women.
Materials and methods: We performed a retrospective cohort analysis using the Consortium on Safe Labor (CSL) database. Women ages 16-45 who were pregnant with singletons and had an obese body mass index (>30 kg/m2) were included in our study population. Multivariable logistic regression was used in order to identify predictors of venous thromboembolism.
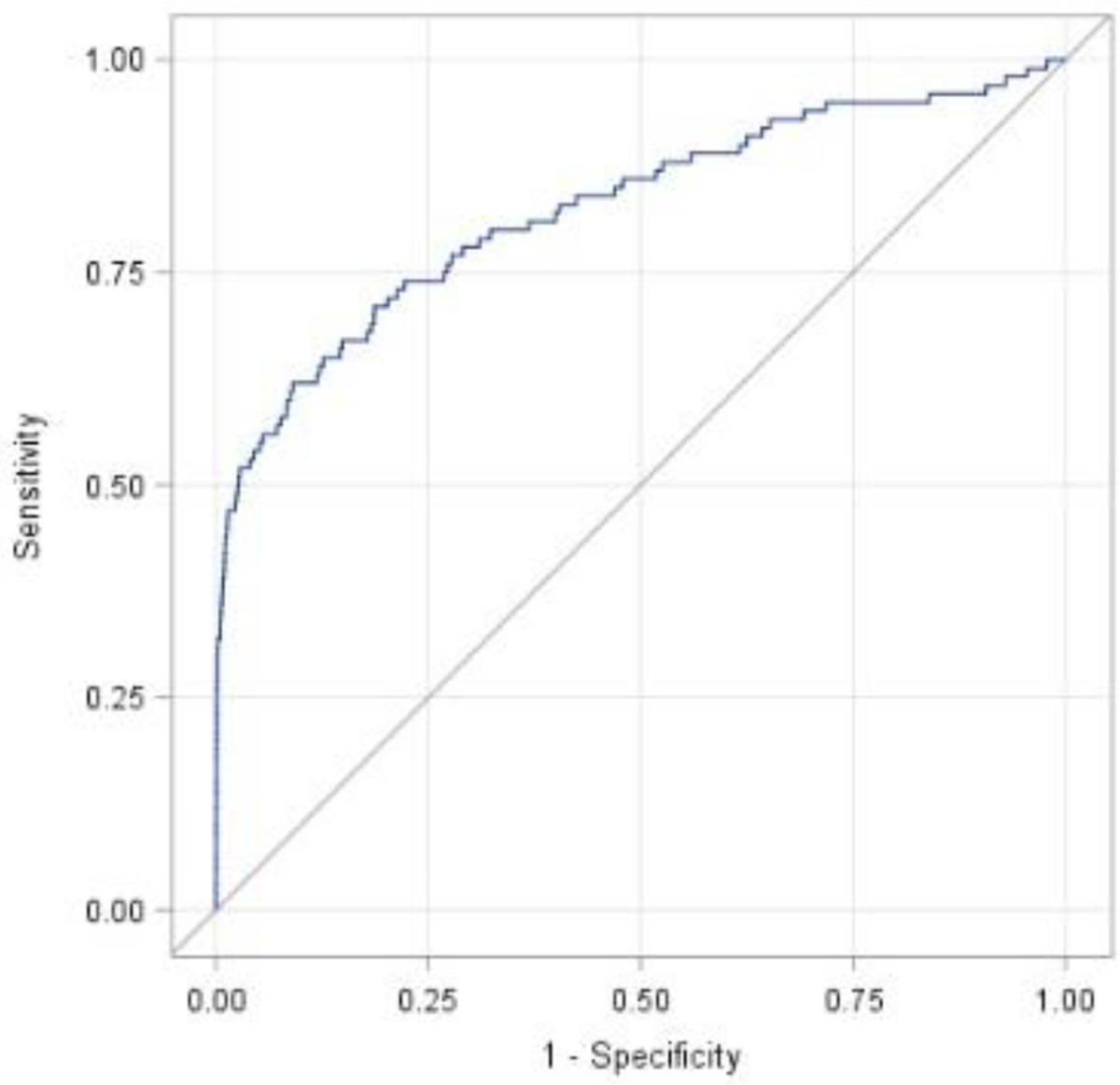
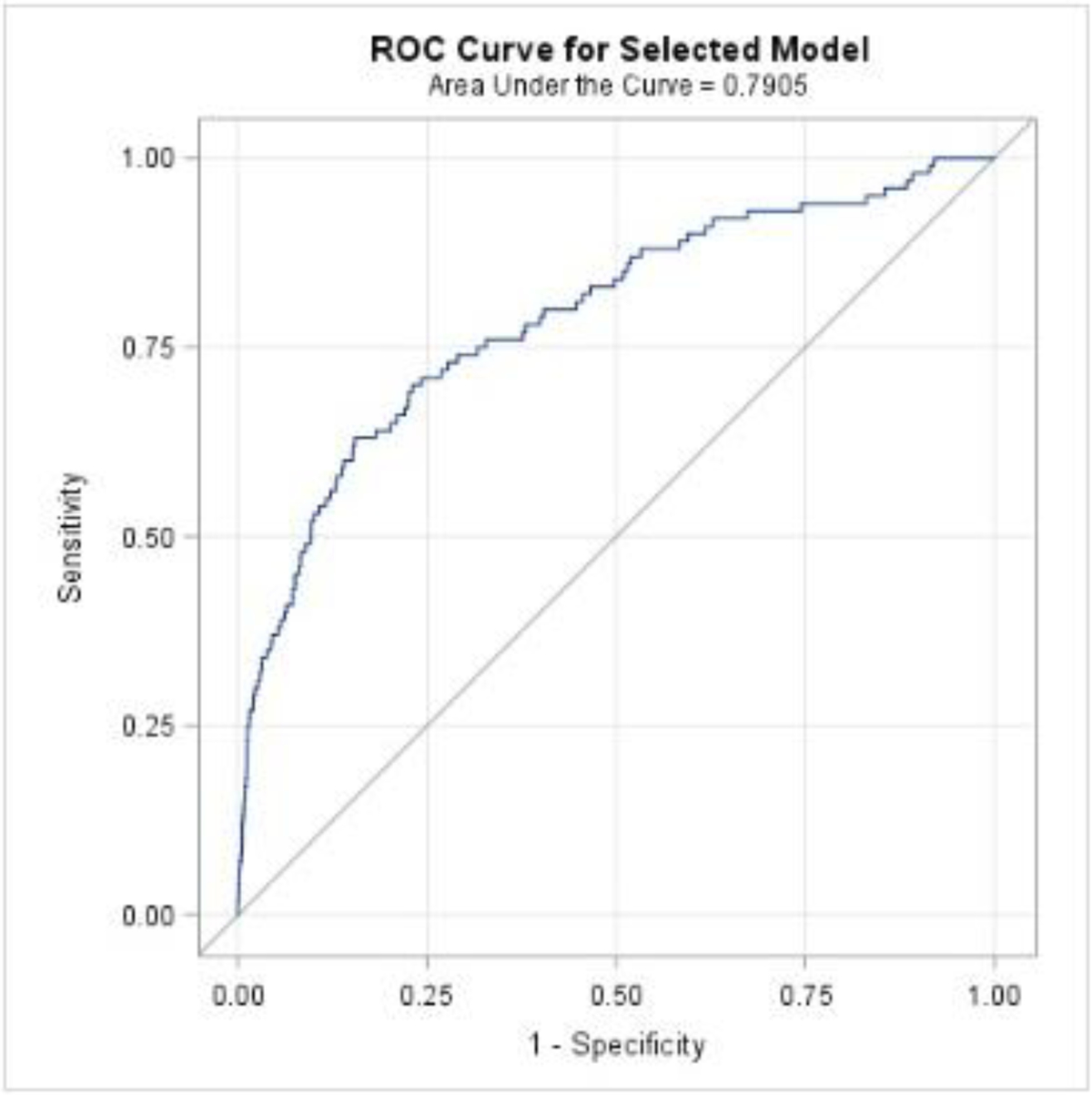
Results: Of the 83,500 women who met inclusion criteria, on average women were 27.8 years old, 38.6 weeks gestation, with body mass index of 35.8, and cesarean delivery incidence of 35.2%. 109 women (0.13%) experienced a VTE event. Independent predictors of VTE in our final multivariable predictive model included: mode of delivery, body mass index, pregestational diabetes, chronic heart disease, preeclampsia, blood transfusion (intrapartum or postpartum), prenatal history of thromboembolic disorder, and postpartum maternal length of stay. A receiver operating characteristic curve was developed to assess the model; area under the curve was 0.826.
Conclusions: We developed a strong predictive model using a large, retrospective database to distinguish risk of VTE in obese pregnant women, which may provide the foundation for future protocol development of obstetrical thromboprophylaxis in obese women.
Keywords: Low molecular weight heparin; Maternal morbidity; Obesity; Pregnancy; Thromboprophylaxis; Venous thromboembolism.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors report no conflict of interest.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
