

Complications and mortality of venovenous extracorporeal membrane oxygenation in the treatment of neonatal respiratory failure: a systematic review and meta-analysis
- PMID: 32380985
- PMCID: PMC7204219
- DOI: 10.1186/s12890-020-1144-8
Complications and mortality of venovenous extracorporeal membrane oxygenation in the treatment of neonatal respiratory failure: a systematic review and meta-analysis
Abstract
Background: Extracorporeal membrane oxygenation (ECMO) has been increasingly used for severe neonatal respiratory failure refractory to conventional treatments. To systematically evaluate the complications and mortality of venovenous ECMO (VV ECMO) in the treatment of neonatal respiratory failure, we performed a systematic review and meta-analysis of all the related studies.
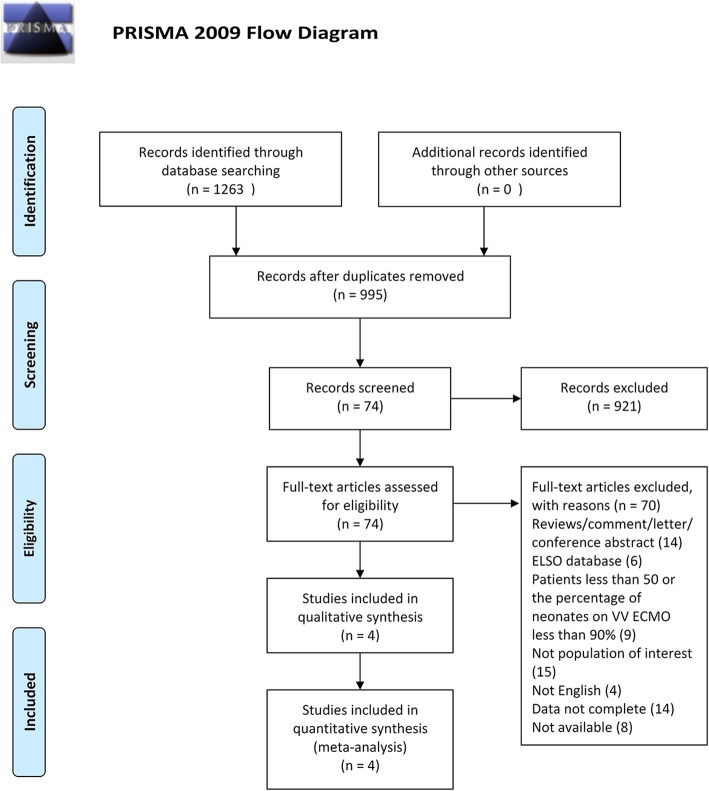
Methods: PubMed, Embase, and Cochrane Library were searched. The retrieval period was from the establishment of the database to February 2019. Two investigators independently screened articles according to the inclusion and exclusion criteria. The quality of article was assessed by the Newcastle-Ottawa scale (NOS). The meta-analysis was performed by Stata 15.0 software.
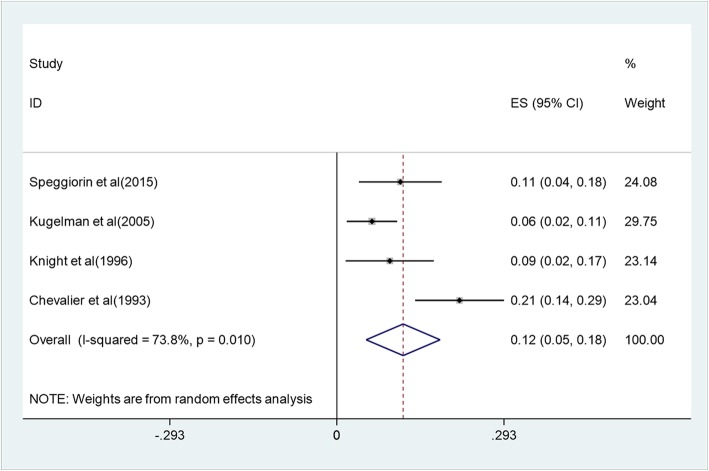
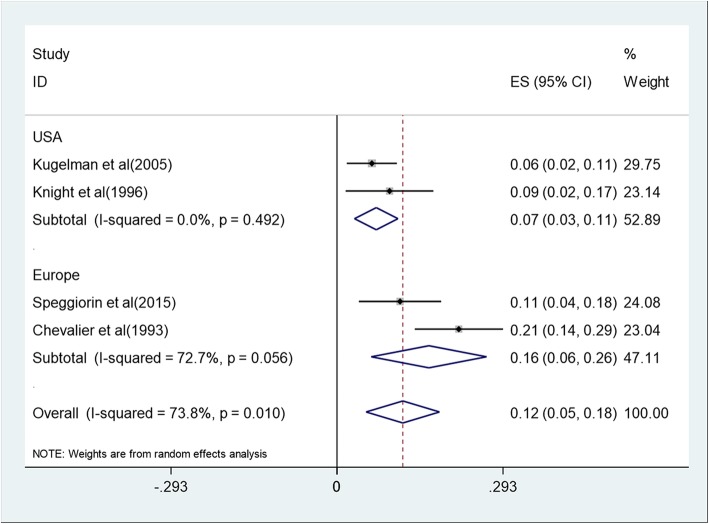
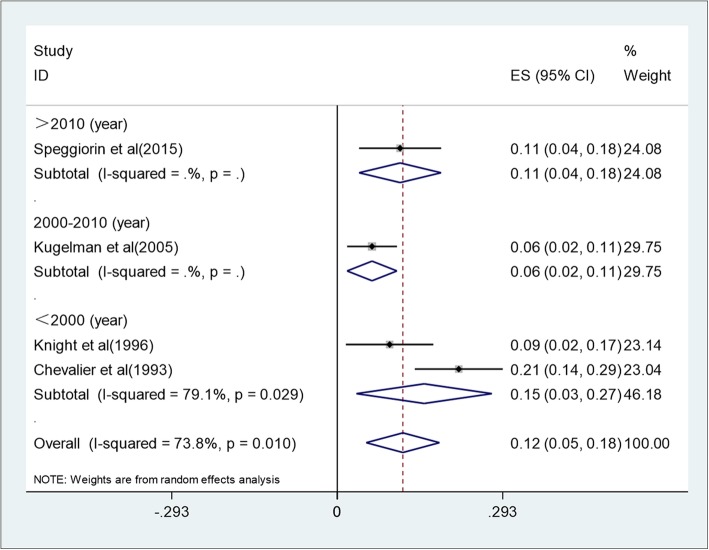
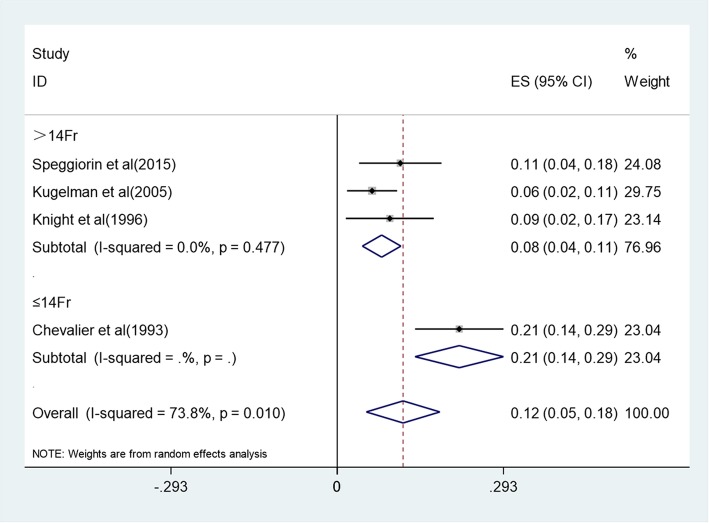
Results: Four observational studies were included, with a total of 347 newborns. VV ECMO was used for neonates with refractory respiratory failure unresponsive to maximal medical therapy. Median ages of the newborns at cannulation were 43.2 h, 23 h, 19 h, and 71 h in the included four studies, respectively. The overall mortality at hospital charge was 12% (5-18%) with a heterogeneity of I2 = 73.8% (p = 0.01). Two studies reported mortality during ECMO and after decannulation, with 10% (0.8-19.2%) and 6.1% (2.6-9.6%), respectively. The most common complications associated with VV ECMO were: pneumothorax (20.6%), hypertension (20.4%), cannula dysfunction (20.2%), seizure (14.9%), renal failure requiring hemofiltration (14.7%), infectious complications (10.3%), thrombi (7.4%), intracranial hemorrhage or infarction (6.6%), hemolysis (5.3%), cannula site bleeding (4.4%), gastrointestinal bleeding (3.7%), oxygenator failure (2.8%), other bleeding events (2.8%), brain death (1.9%), and myocardial stun (0.9%).
Conclusion: The overall mortality at discharge of VV ECMO in the treatment of neonatal respiratory failure was 12%. Although complications are frequent, the survival rate during hospitalization is still high. Further larger samples, and higher quality of randomized controlled trials (RCTs) are needed to clarify the efficacy and safety of this technique in the treatment of neonatal respiratory failure.
Keywords: Extracorporeal membrane oxygenation; Meta-analysis; Neonate; Respiratory failure; Systematic reviews.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
