

Prognosis of unrecognised myocardial infarction determined by electrocardiography or cardiac magnetic resonance imaging: systematic review and meta-analysis
- PMID: 32381490
- PMCID: PMC7203874
- DOI: 10.1136/bmj.m1184
Prognosis of unrecognised myocardial infarction determined by electrocardiography or cardiac magnetic resonance imaging: systematic review and meta-analysis
Abstract
Objective: To evaluate the prognosis of unrecognised myocardial infarction determined by electrocardiography (UMI-ECG) or cardiac magnetic resonance imaging (UMI-CMR).
Design: Systematic review and meta-analysis of prospective studies.
Data sources: Electronic databases, including PubMed, Embase, and Google Scholar.
Study selection: Prospective cohort studies were included if they reported adjusted relative risks, odds ratios, or hazard ratios and 95% confidence intervals for all cause mortality or cardiovascular outcomes in participants with unrecognised myocardial infarction compared with those without myocardial infarction.
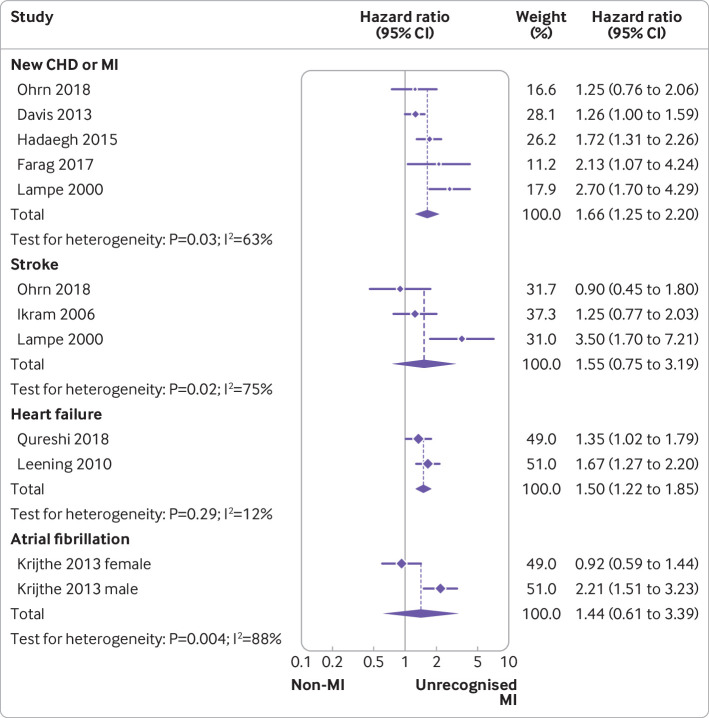
Data extraction and synthesis: The primary outcomes were composite major adverse cardiac events, all cause mortality, and cardiovascular mortality associated with UMI-ECG and UMI-CMR. The secondary outcomes were the risks of recurrent coronary heart disease or myocardial infarction, stroke, heart failure, and atrial fibrillation. Pooled hazard ratios and 95% confidence intervals were reported. The heterogeneity of outcomes was compared in clinically recognised and unrecognised myocardial infarction.
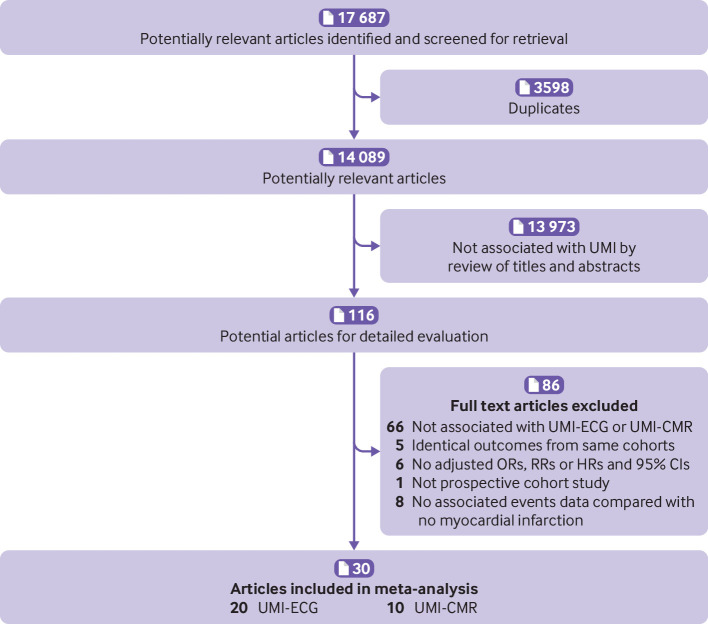
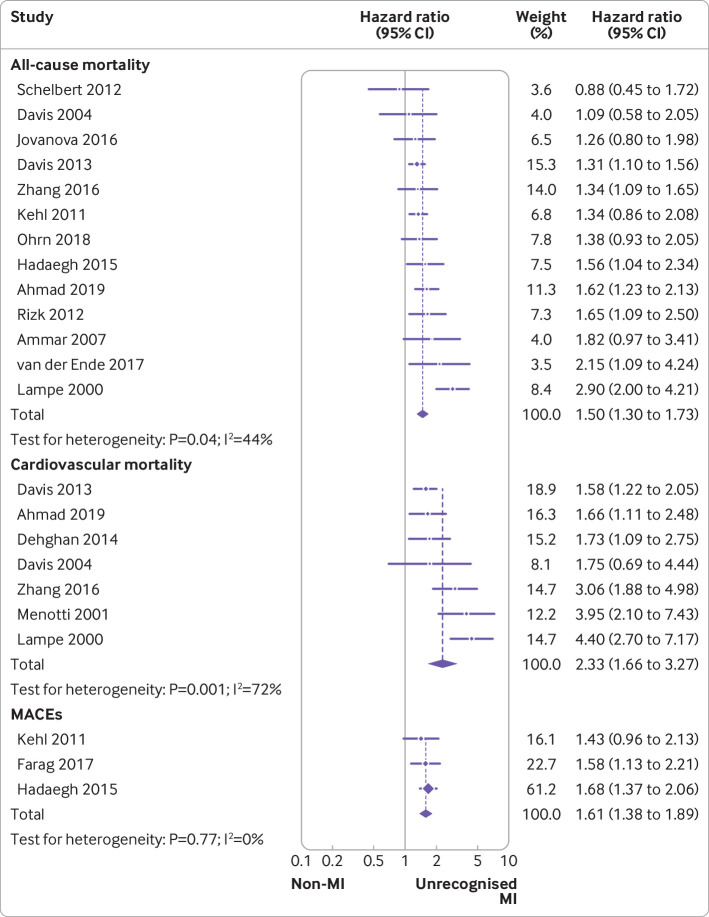
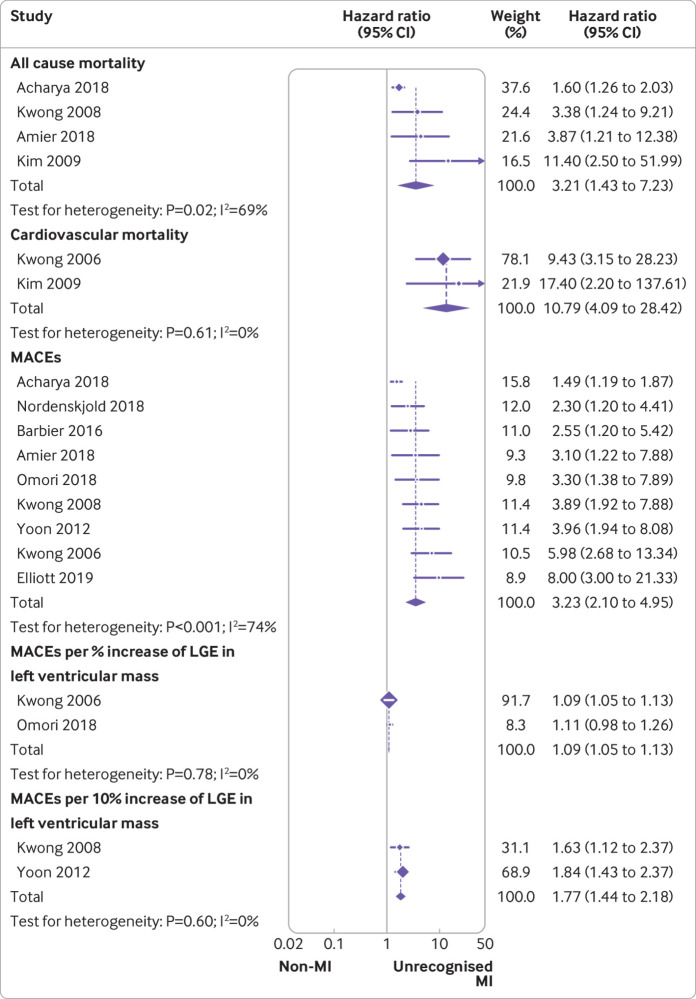
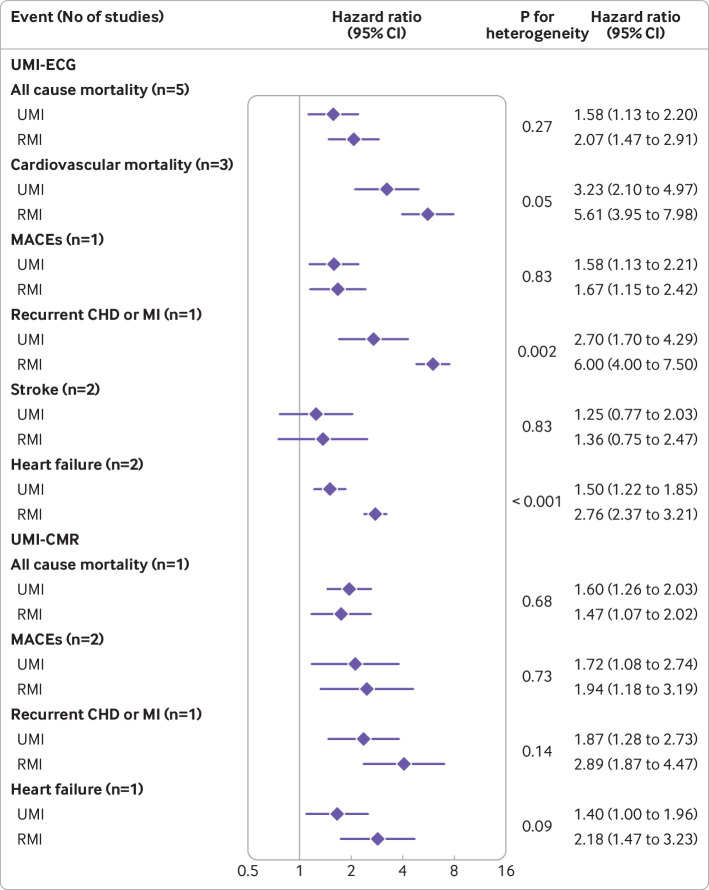
Results: The meta-analysis included 30 studies with 253 425 participants and 1 621 920 person years of follow-up. UMI-ECG was associated with increased risks of all cause mortality (hazard ratio 1.50, 95% confidence interval 1.30 to 1.73), cardiovascular mortality (2.33, 1.66 to 3.27), and major adverse cardiac events (1.61, 1.38 to 1.89) compared with the absence of myocardial infarction. UMI-CMR was also associated with increased risks of all cause mortality (3.21, 1.43 to 7.23), cardiovascular mortality (10.79, 4.09 to 28.42), and major adverse cardiac events (3.23, 2.10 to 4.95). No major heterogeneity was observed for any primary outcomes between recognised myocardial infarction and UMI-ECG or UMI-CMR. The absolute risk differences were 7.50 (95% confidence interval 4.50 to 10.95) per 1000 person years for all cause mortality, 11.04 (5.48 to 18.84) for cardiovascular mortality, and 27.45 (17.1 to 40.05) for major adverse cardiac events in participants with UMI-ECG compared with those without myocardial infarction. The corresponding data for UMI-CMR were 32.49 (6.32 to 91.58), 37.2 (11.7 to 104.20), and 51.96 (25.63 to 92.04), respectively.
Conclusions: UMI-ECG or UMI-CMR is associated with an adverse long term prognosis similar to that of recognised myocardial infarction. Screening for unrecognised myocardial infarction could be useful for risk stratification among patients with a high risk of cardiovascular disease.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Natural Science Foundation of China, Science and Technology Innovation Project from Foshan, Guangdong, and Shunde Hospital, Southern Medical University for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical