

Association of physician payment model and team-based care with timely access in primary care: a population-based cross-sectional study
- PMID: 32381684
- PMCID: PMC7207031
- DOI: 10.9778/cmajo.20190063
Association of physician payment model and team-based care with timely access in primary care: a population-based cross-sectional study
Abstract
Background: It is unclear how patient-reported access to primary care differs by physician payment model and participation in team-based care. We examined the association between timely and after-hours access to primary care and physician payment model and participation in team-based care, and sought to assess how access varied by patient characteristics.
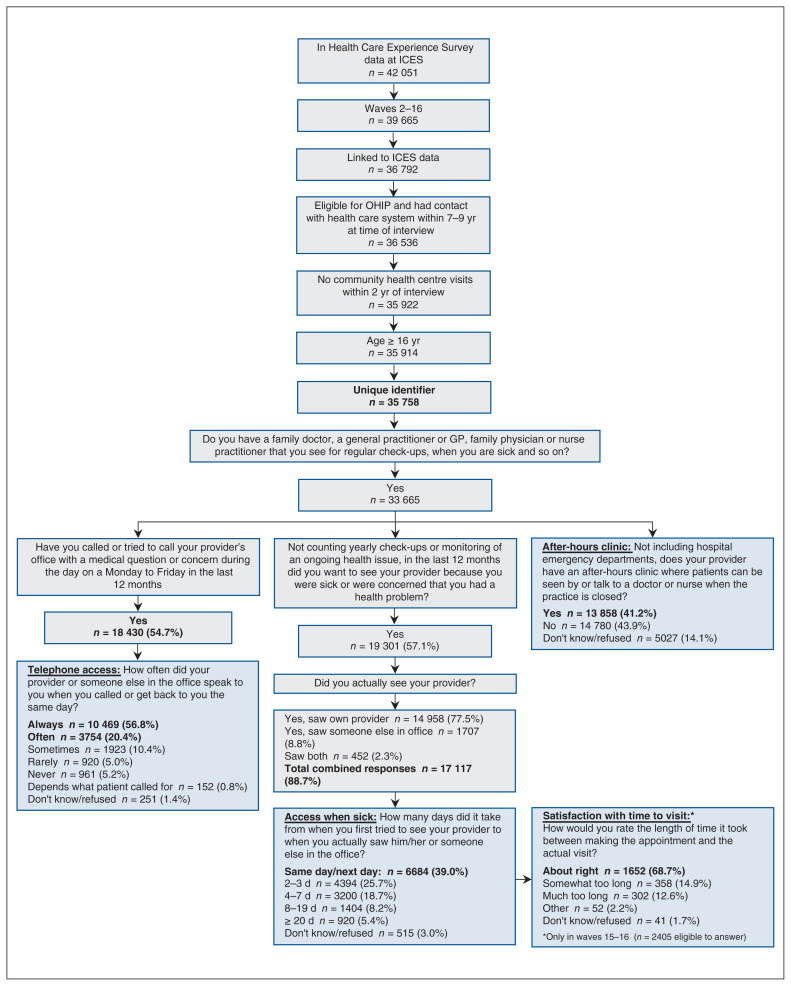
Methods: We conducted a cross-sectional analysis of adult (age ≥ 16 yr) Ontarians who responded to the Ontario Health Care Experience Survey between January 2013 and September 2015, reported having a primary care provider and agreed to have their responses linked to health administrative data. Access measures included the proportion of respondents who reported same-day or next-day access when sick, satisfaction with time to appointment when sick, telephone access and knowledge of an after-hours clinic. We tested the association between practice model and measures of access using logistic regression after stratifying for rurality.
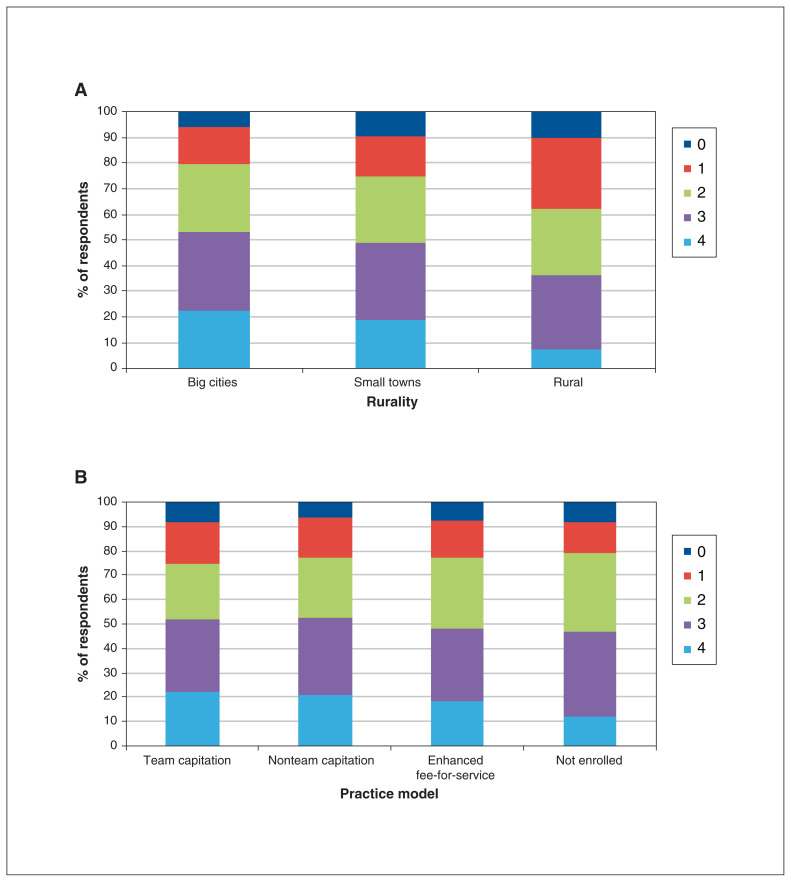
Results: A total of 33 665 respondents met our inclusion criteria. In big cities, respondents in team and nonteam capitation models were less likely to report same-day or next-day access when sick than respondents in enhanced fee-for-service models (team capitation 43%, adjusted odds ratio [OR] 0.88, 95% confidence interval [CI] 0.79-0.98; nonteam capitation 39%, adjusted OR 0.78, 95% CI 0.70-0.87; enhanced fee-for-service 46% [reference]). Respondents in team and nonteam capitation models were more likely than those in enhanced fee-for-service models to report that their provider had an after-hours clinic (team capitation 59%, adjusted OR 2.59, 95% CI 2.39-2.81; nonteam capitation 51%, adjusted OR 1.90, 95% CI 1.76-2.04; enhanced fee-for service 34% [reference]). Patterns were similar for respondents in small towns. There was minimal to no difference by model for satisfaction with time to appointment or telephone access.
Interpretation: In our setting, there was an association between some types of access to primary care and physician payment model and team-based care, but the direction was not consistent. Different measures of timely access are needed to understand health care system performance.
Copyright 2020, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Tara Kiran was the Board Chair for the St. Michael’s Hospital Academic Family Health Team from 2014 to 2018. No other competing interests were declared.
Figures

References
-
- Starfield B. Primary care: balancing health needs, services, and technology. Oxford (UK): Oxford University Press; 1998.
-
- How Canada compares: results from the Commonwealth Fund’s 2016 international health policy survey of adults in 11 countries. Ottawa: Canadian Institute for Health Information; 2017.
-
- Iglehart JK. No place like home — testing a new model of care delivery. N Engl J Med. 2008;359:1200–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous