

Immune-related adverse events of checkpoint inhibitors
- PMID: 32382051
- PMCID: PMC9728094
- DOI: 10.1038/s41572-020-0160-6
Immune-related adverse events of checkpoint inhibitors
Abstract
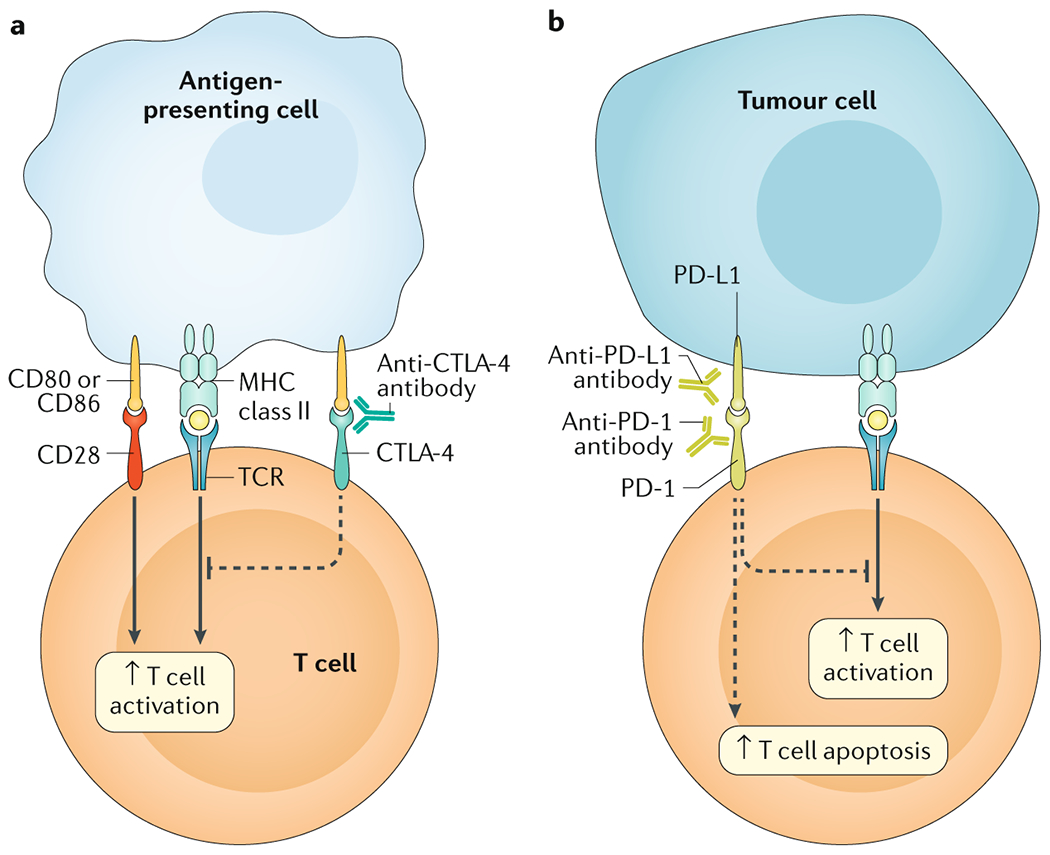
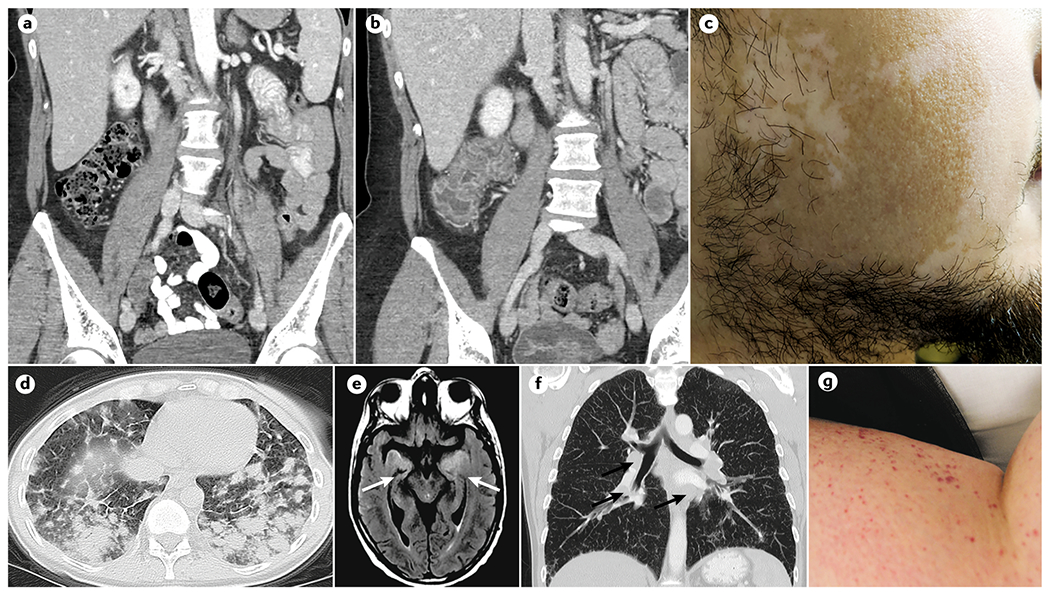
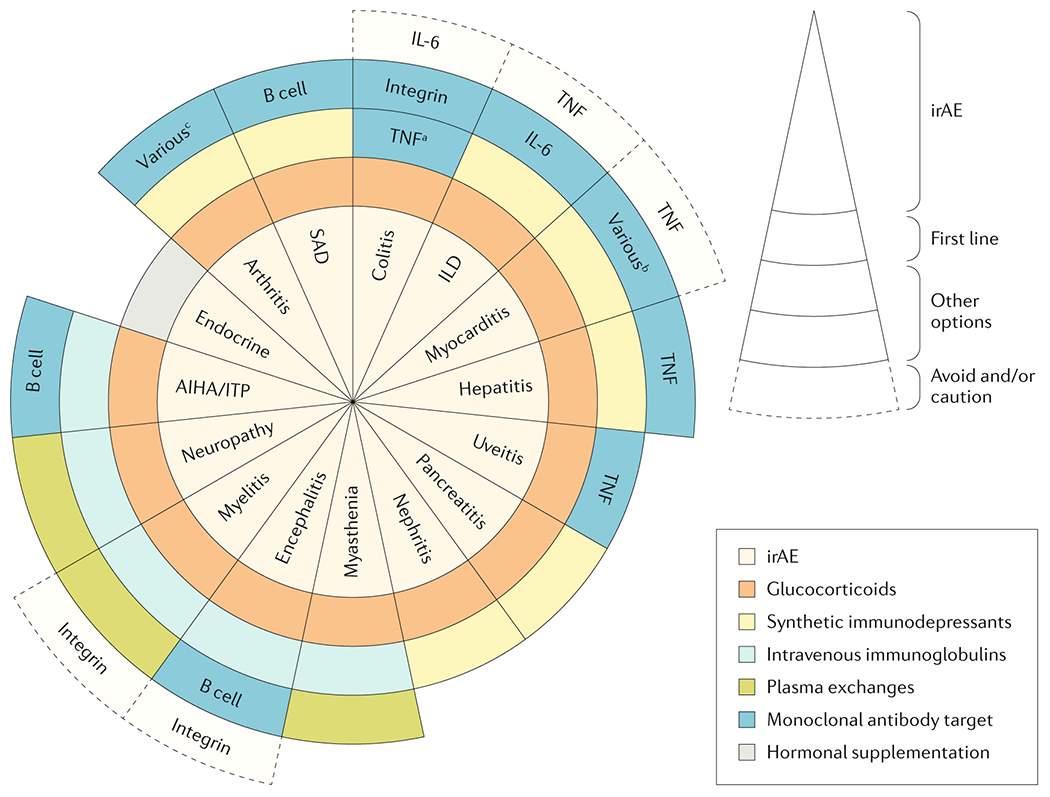
Cancer immunotherapies have changed the landscape of cancer treatment during the past few decades. Among them, immune checkpoint inhibitors, which target PD-1, PD-L1 and CTLA-4, are increasingly used for certain cancers; however, this increased use has resulted in increased reports of immune-related adverse events (irAEs). These irAEs are unique and are different to those of traditional cancer therapies, and typically have a delayed onset and prolonged duration. IrAEs can involve any organ or system. These effects are frequently low grade and are treatable and reversible; however, some adverse effects can be severe and lead to permanent disorders. Management is primarily based on corticosteroids and other immunomodulatory agents, which should be prescribed carefully to reduce the potential of short-term and long-term complications. Thoughtful management of irAEs is important in optimizing quality of life and long-term outcomes.
Figures

References
-
- Hoos A Development of immuno-oncology drugs - from CTLA4 to PD1 to the next generations. Nat. Rev. Drug Discov 15, 235–247 (2016). - PubMed
-
- Postow MA, Sidlow R & Hellmann MD Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med 378, 158–168 (2018). - PubMed
-
One of the first central reviews surveying the irAEs associated with ICIs and their management.
-
- Ramos-Casals M et al. Immune-Related Adverse Events Induced By Cancer Immunotherapies. Big Data Analysis of 13,051 cases (ImmunoCancer International Registry). Ann. Rheum. Dis (2019).
-
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). (2019).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
