

Anaplastic meningioma seeding of the abdominal wall following calvarial bone flap preservation
- PMID: 32382362
- PMCID: PMC7198915
- DOI: 10.1016/j.radcr.2020.03.004
Anaplastic meningioma seeding of the abdominal wall following calvarial bone flap preservation
Abstract
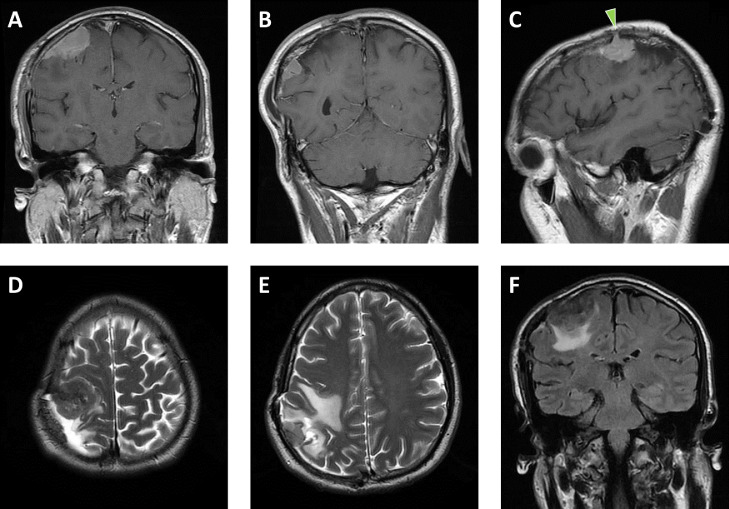
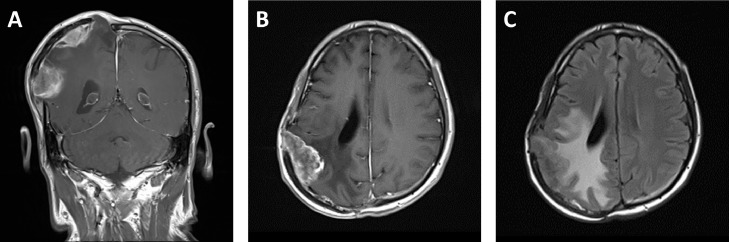
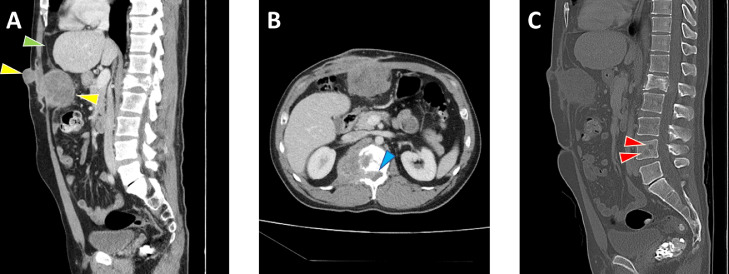
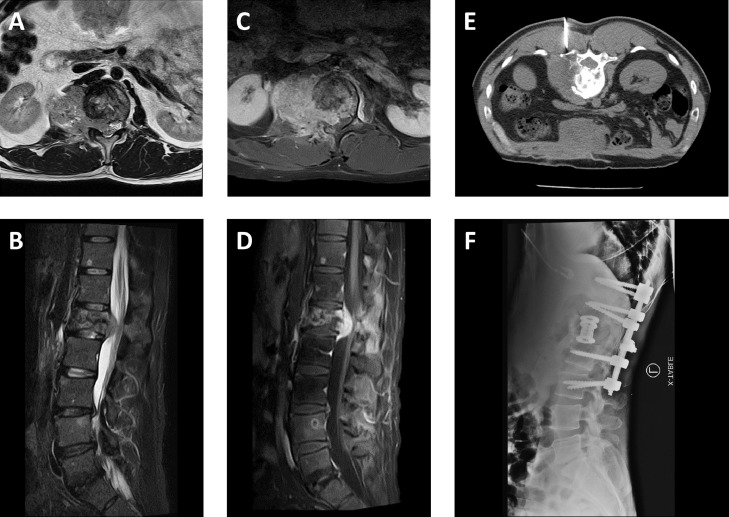
Meningiomas are common intracranial tumors that rarely metastasize. We present a highly unusual case of a 42-year-old man with direct seeding of meningioma to the abdominal wall. The patient had a history of multiple operations for a recurrent intracranial meningioma with decompressive craniectomy and preservation of the calvarial bone flap by implantation into the subcutaneous layer of the anterior abdominal wall. Following removal of the bone flap, a new abdominal wall mass was identified, consistent with iatrogenic implantation of anaplastic meningioma.
Keywords: Anaplastic meningioma; Calvarial bone flap preservation; Central nervous system neoplasms; Metastatic meningioma.
© 2020 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
Similar articles
-
Giant malignant meningioma invading the calvarial bone and scalp.J Craniofac Surg. 2012 Mar;23(2):599-602. doi: 10.1097/SCS.0b013e31824cd718. J Craniofac Surg. 2012. PMID: 22446424
-
Bone Flap Conservation in the Scalp After Decompressive Craniectomy.World Neurosurg. 2018 Dec;120:e269-e273. doi: 10.1016/j.wneu.2018.08.048. Epub 2018 Aug 20. World Neurosurg. 2018. PMID: 30138734
-
Iatrogenic implantation of malignant meningioma to the abdominal wall.Virchows Arch. 2001 Mar;438(3):316-8. doi: 10.1007/s004280000347. Virchows Arch. 2001. PMID: 11315631
-
Anaplastic meningioma: case report.Arq Neuropsiquiatr. 2001 Dec;59(4):939-43. doi: 10.1590/s0004-282x2001000600019. Arq Neuropsiquiatr. 2001. PMID: 11733842 Review.
-
Childhood intracranial meningiomas after high-dose irradiation.Cancer. 1993 Jun 15;71(12):4091-5. doi: 10.1002/1097-0142(19930615)71:12<4091::aid-cncr2820711247>3.0.co;2-g. Cancer. 1993. PMID: 8508374 Review.
Cited by
-
Complete loss of E-cadherin expression in a rare case of metastatic malignant meningioma: a case report.BMC Neurol. 2023 Nov 4;23(1):398. doi: 10.1186/s12883-023-03450-w. BMC Neurol. 2023. PMID: 37925427 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
