

What is the validity of self-reported fractures?
- PMID: 32382588
- PMCID: PMC7200867
- DOI: 10.1016/j.bonr.2020.100256
What is the validity of self-reported fractures?
Abstract
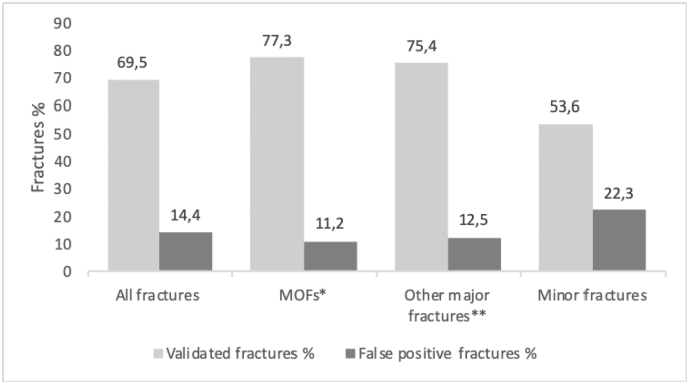
We assessed the validity of self-reported fractures, over a median follow-up period of 6.2 years, in a well characterized population-based cohort of 3560 postmenopausal women, aged 60-85 years, from the Fracture Risk Brussels Epidemiological Enquiry (FRISBEE) study. Incident low-traumatic (falls from a standing height or less) or non-traumatic fractures, including peripheral fractures, were registered during each annual follow-up telephone interview. A self-reported fracture was considered as a true positive if it was validated by written reliable medical reports (radiographs, CT scans or surgical report). False positives fractures were considered to be those for which the radiology report indicated that there was no fracture at the reported site. Among self-reported fractures, false positive rates were 14.4% for all fractures. The rate of false positives of 11.2% (n = 48/429) was not negligible for the four classical major osteoporotic fractures (MOFs: hip, clinical spine, forearm or shoulder fractures). In terms of fracture site, we found the lowest false positive rate (4.4%) at the hip, and the highest (16.8%) at the spine, with the proximal humerus and the wrist in between, at about 10% each. The global rates of false positives were 12.5% (n = 22/176) for other major fractures and 22.3% (n = 49/220) for minor fractures. Younger subjects, individuals with fractures at sites other than the hip, with a lower education level, or with a higher BMI were more likely to report false positive fractures. Our data indicate that the inaccuracy of self-reported fractures is clinically relevant for several major fractures, which could influence any fracture risk prediction model.
Keywords: Epidemiology; False positives; Fractures; Osteoporosis; Self-report.
© 2020 The Authors.
Conflict of interest statement
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
Figures


References
-
- Beard C.M., Melton L.J., III, Cedel S.L., Richelson L.S., Riggs B.L. Ascertainment of risk factors for osteoporosis: comparison of interview data with medical record review. J. Bone Miner. Res. 1990;5:691–699. - PubMed
-
- Cappelle S.I., Ramon I., Dekelver C., Rozenberg S., Baleanu F., Karmali R., Rubinstein M., Tondeur M., Moreau M., Paesmans M., Bergmann P., Body J.J. Distribution of clinical risk factors for fracture in a Brussels cohort of postmenopausal women: the FRISBEE study and comparison with other major cohort studies. Maturitas. 2017;106:1–7. - PubMed
-
- Chen Z., Kooperberg C., Pettinger M.B., Bassford T., Cauley J.A., LaCroix A.Z., Lewis C.E., Kipersztok S., Borne C., Jackson R.D. Validity of self-report for fractures among a multiethnic cohort of postmenopausal women: results from the Women’s Health Initiative observational study and clinical trials. Menopause. 2004;11:264–274. - PubMed
-
- Colditz G.A., Martin P., Stampfer M.J., Willett W.C., Sampson L., Rosner B., Hennekens C.H., Speizer F.E. Validation of questionnaire information on risk factors and disease outcomes in a prospective cohort study of women. Am. J. Epidemiol. 1986;123:894–900. - PubMed
LinkOut - more resources
Full Text Sources
