

Etiologies of Proptosis: A review
- PMID: 32382689
- PMCID: PMC7204542
- DOI: 10.18103/imr.v6i3.852
Etiologies of Proptosis: A review
Abstract
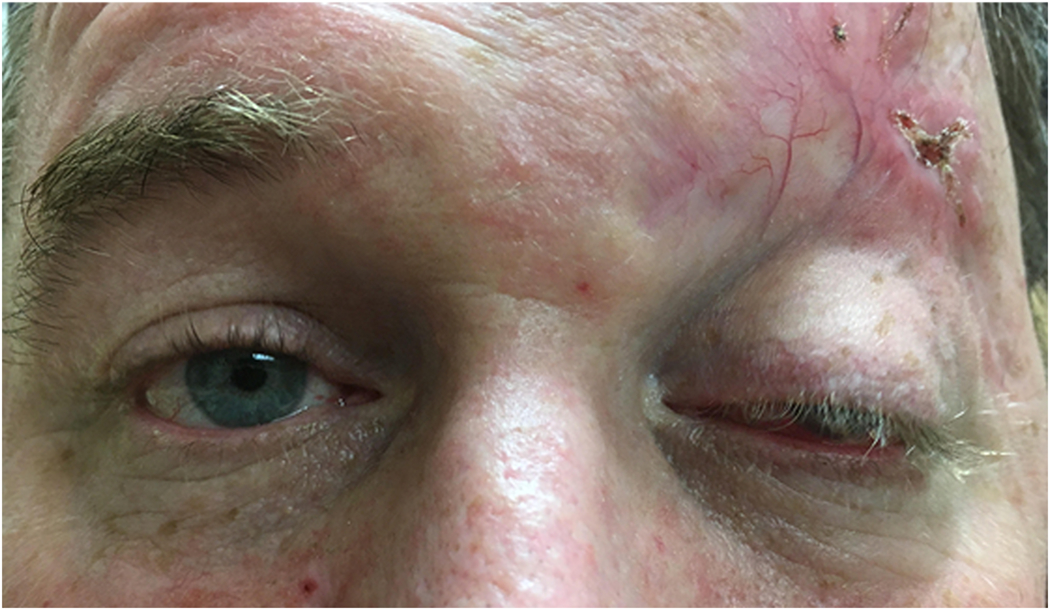
Proptosis, the protrusion of the eyeball from the orbit, results from a wide variety of pathologies that can be vision- or life-threatening. Clinical history, associated physical exam findings, and imaging features are all crucial in establishing the underlying etiology. The differential diagnosis is broad, and includes infectious, inflammatory, vascular, and neoplastic entities that range from benign and indolent, to malignant and aggressive. While treatment varies significantly based on the disease process, all are aimed at preserving vision, salvaging the globe, preventing disfigurement, and reducing mortality. Both internists and general ophthalmologists should be familiar with the causes of proptosis in order to initiate the work-up for, and appropriately triage, affected patients.
Keywords: Proptosis; orbital infection; orbital inflammation; orbital tumors; orbital vascular anomalies.
Figures




References
-
- Rootman J Diseases of the Orbit: A Multidisciplinary Approach. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2003.
-
- Dutton JJ. Atlas of Clinical and Surgical Orbital Anatomy. 2nd ed. Philadelphia: Elsevier Saunders; 2011.
-
- Aviv RI, Casselman J. Orbital imaging: Part 1. Normal anatomy Clin Radiol. 2005. March;60(3):279–87. - PubMed
-
- Conneely MF, Hacein-Bey L, Jay WM. Magnetic resonance imaging of the orbit. Semin Ophthalmol. 2008. May-Jun;23(3): 179–89. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources