

IPNA clinical practice recommendations for the diagnosis and management of children with steroid-resistant nephrotic syndrome
- PMID: 32382828
- PMCID: PMC7316686
- DOI: 10.1007/s00467-020-04519-1
IPNA clinical practice recommendations for the diagnosis and management of children with steroid-resistant nephrotic syndrome
Abstract
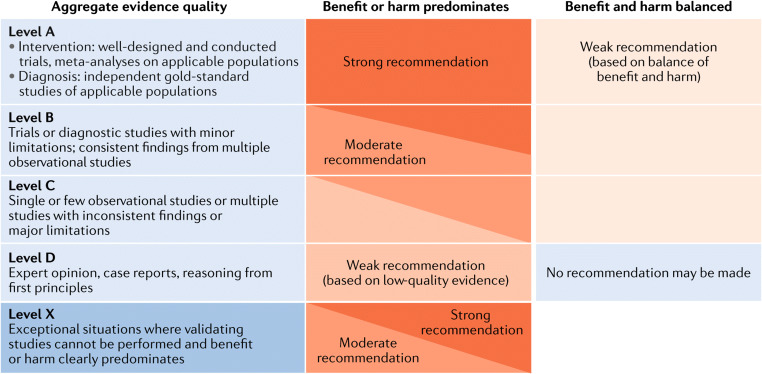
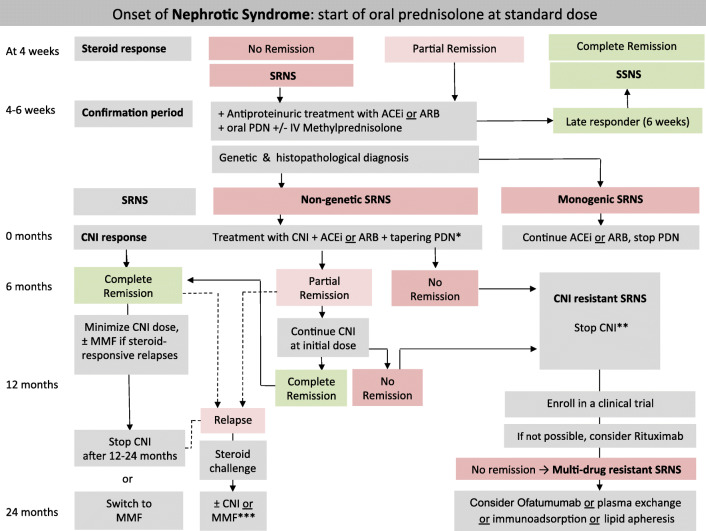
Idiopathic nephrotic syndrome newly affects 1-3 per 100,000 children per year. Approximately 85% of cases show complete remission of proteinuria following glucocorticoid treatment. Patients who do not achieve complete remission within 4-6 weeks of glucocorticoid treatment have steroid-resistant nephrotic syndrome (SRNS). In 10-30% of steroid-resistant patients, mutations in podocyte-associated genes can be detected, whereas an undefined circulating factor of immune origin is assumed in the remaining ones. Diagnosis and management of SRNS is a great challenge due to its heterogeneous etiology, frequent lack of remission by further immunosuppressive treatment, and severe complications including the development of end-stage kidney disease and recurrence after renal transplantation. A team of experts including pediatric nephrologists and renal geneticists from the International Pediatric Nephrology Association (IPNA), a renal pathologist, and an adult nephrologist have now developed comprehensive clinical practice recommendations on the diagnosis and management of SRNS in children. The team performed a systematic literature review on 9 clinically relevant PICO (Patient or Population covered, Intervention, Comparator, Outcome) questions, formulated recommendations and formally graded them at a consensus meeting, with input from patient representatives and a dietician acting as external advisors and a voting panel of pediatric nephrologists. Research recommendations are also given.
Keywords: Children; Chronic kidney disease; Genetics; Immunosuppressive treatment; Outcome; Pediatrics; Steroid-resistant nephrotic syndrome.
Conflict of interest statement
D.H. has received research grants from Kyowa Kirin and Amgen, and has received speaker and/or consultant fees from Amgen, Sandoz, Kyowa Kirin, Pfizer, Merck Serono, Horizon, and Chiesi. O.B. has received speaker and/or consultant fees from Amgen, Chiesi, Novartis, and Octapharma. These were all unrelated to the topic of this guideline. The other authors declare no competing interests.
Figures
References
-
- Noone DG, Iijima K, Parekh R. Idiopathic nephrotic syndrome in children. Lancet. 2018;392(10141):61–74. - PubMed
-
- Eddy AA, Symons JM. Nephrotic syndrome in childhood. Lancet. 2003;362(9384):629–639. - PubMed
-
- McKinney PA, Feltbower RG, Brocklebank JT, Fitzpatrick MM. Time trends and ethnic patterns of childhood nephrotic syndrome in Yorkshire, UK. Pediat Nephrol (Berlin, Germany) 2001;16(12):1040–1044. - PubMed
-
- Dossier C, Lapidus N, Bayer F, Sellier-Leclerc AL, Boyer O, de Pontual L, May A, Nathanson S, Orzechowski C, Simon T, Carrat F, Deschenes G. Epidemiology of idiopathic nephrotic syndrome in children: endemic or epidemic? Pediat Nephrol (Berlin, Germany) 2016;31(12):2299–2308. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
