

Epidemiological trends of surgical admissions to the intensive care unit in the United States
- PMID: 32384370
- PMCID: PMC7799916
- DOI: 10.1097/TA.0000000000002768
Epidemiological trends of surgical admissions to the intensive care unit in the United States
Abstract
Background: Epidemiologic assessment of surgical admissions into intensive care units (ICUs) provides a framework to evaluate health care system efficiency and project future health care needs.
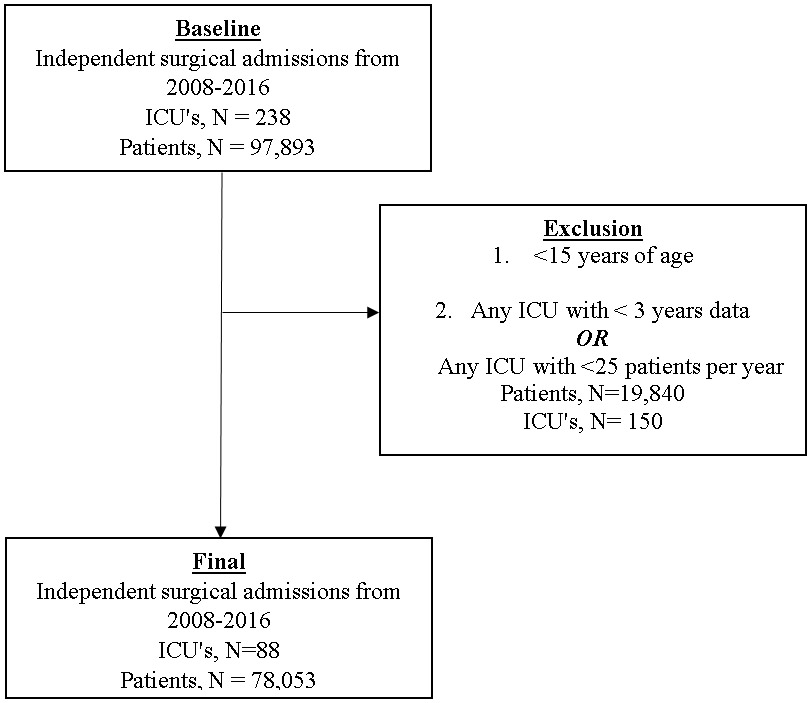
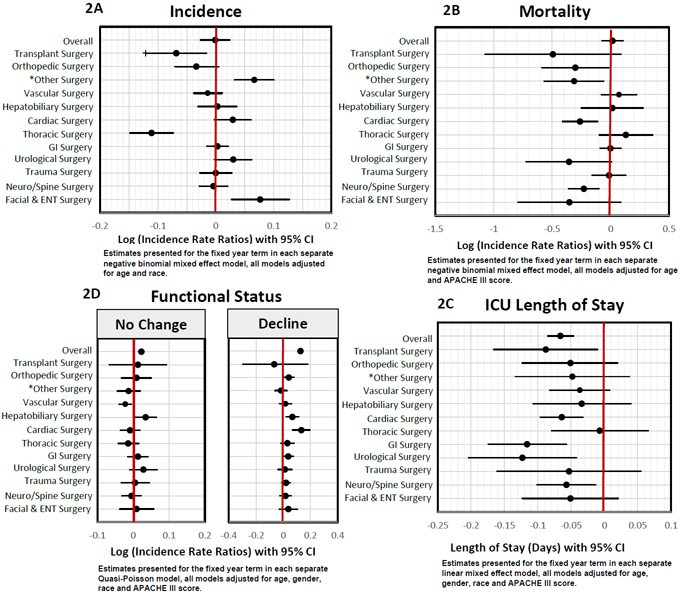
Methods: We performed a 9-year (2008-2016), retrospective, cohort analysis of all adult admissions to 88 surgical ICUs using the prospectively and manually abstracted Cerner Acute Physiology and Chronic Health Evaluation Outcomes database. We stratified patients into 13 surgical cohorts and modeled temporal trends in admission, mortality, surgical ICU length of stay (LOS), and change in functional status (FS) using generalized mixed-effects and Quasi-Poisson models to obtain risk-adjusted outcomes.
Results: We evaluated 78,053 ICU admissions and observed a significant decrease in admissions after transplant and thoracic surgery, with a concomitant increase in admissions after otolaryngological and facial reconstructive procedures (all p < 0.05). While overall risk-adjusted mortality remained stable over the study period; mortality significantly declined in orthopedic, cardiac, urologic, and neurosurgical patients (all p < 0.05). Cardiac, urologic, gastrointestinal, neurosurgical, and orthopedic admissions showed significant reductions in LOS (all p < 0.05). The overall rate of FS deterioration increased per year, suggesting ICU-related disability increased over the study period.
Conclusion: Temporal analysis demonstrates a significant change in the type of surgical patients admitted to the ICU over the last decade, with decreasing mortality and LOS in selected cohorts, but an increasing rate of FS deterioration. Improvement in ICU outcomes may highlight the success of health care advancements within certain surgical cohorts, while simultaneously identifying cohorts that may benefit from future intervention. Our findings have significant implications in health care systems planning, including resource and personnel allocation, education, and surgical training.
Level of evidence: Economic/decision, level IV.Epidemiologic, level IV.
Conflict of interest statement
Disclosures and Conflicts of Interest
Victor Vakayil, MBBS, MS - None
Nicholas E. Ingraham, MD - None
Alexandria J. Robbins, MD - None
Rebecca Freese, MS - None
Elise F. Northrop, BA - None
Kathryn Pendleton, MD - None
Melissa Brunsvold, MD - None
Anthony Charles, MD, MPH – None
Jeffrey G. Chipman, MD - None
Christopher J. Tignanelli, MD – None
Figures
References
-
- Halpern NA, Pastores SM, Greenstein RJ. Critical care medicine in the United States 1985-2000: an analysis of bed numbers, use, and costs. Crit Care Med. 2004. June;32(6):1254–9. - PubMed
-
- Halpern NA, Pastores SM, Thaler HT, Greenstein RJ. Changes in critical care beds and occupancy in the United States 1985-2000: Differences attributable to hospital size. Crit Care Med. 2006. August;34(8):2105–12. - PubMed
-
- Halpern NA, Pastores SM. Critical care medicine in the United States 2000-2005: an analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med. 2010. January;38(1):65–71. - PubMed
-
- Wallace DJ, Angus DC, Seymour CW, Barnato AE, Kahn JM. Critical care bed growth in the United States. A comparison of regional and national trends. Am J Respir Crit Care Med. 2015. February 15;191(4):410–6. Available from: https://www.ncbi.nlm.nih.gov/pubmed/25522054 - PMC - PubMed
-
- Wallace DJ, Seymour CW, Kahn JM. Hospital-Level Changes in Adult ICU Bed Supply in the United States. Crit Care Med. 2017. January;45(1):e67–76. Available from: https://www.ncbi.nlm.nih.gov/pubmed/27661861 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
