

Systematic review of patient-oriented interventions to reduce unnecessary use of antibiotics for upper respiratory tract infections
- PMID: 32384919
- PMCID: PMC7210679
- DOI: 10.1186/s13643-020-01359-w
Systematic review of patient-oriented interventions to reduce unnecessary use of antibiotics for upper respiratory tract infections
Abstract
Background: Antibiotics are prescribed frequently for upper respiratory tract infections (URTIs) even though most URTIs do not require antibiotics. This over-prescription contributes to antibiotic resistance which is a major health problem globally. As physicians' prescribing behaviour is influenced by patients' expectations, there may be some opportunities to reduce antibiotic prescribing using patient-oriented interventions. We aimed to identify these interventions and to understand which ones are more effective in reducing unnecessary use of antibiotics for URTIs.
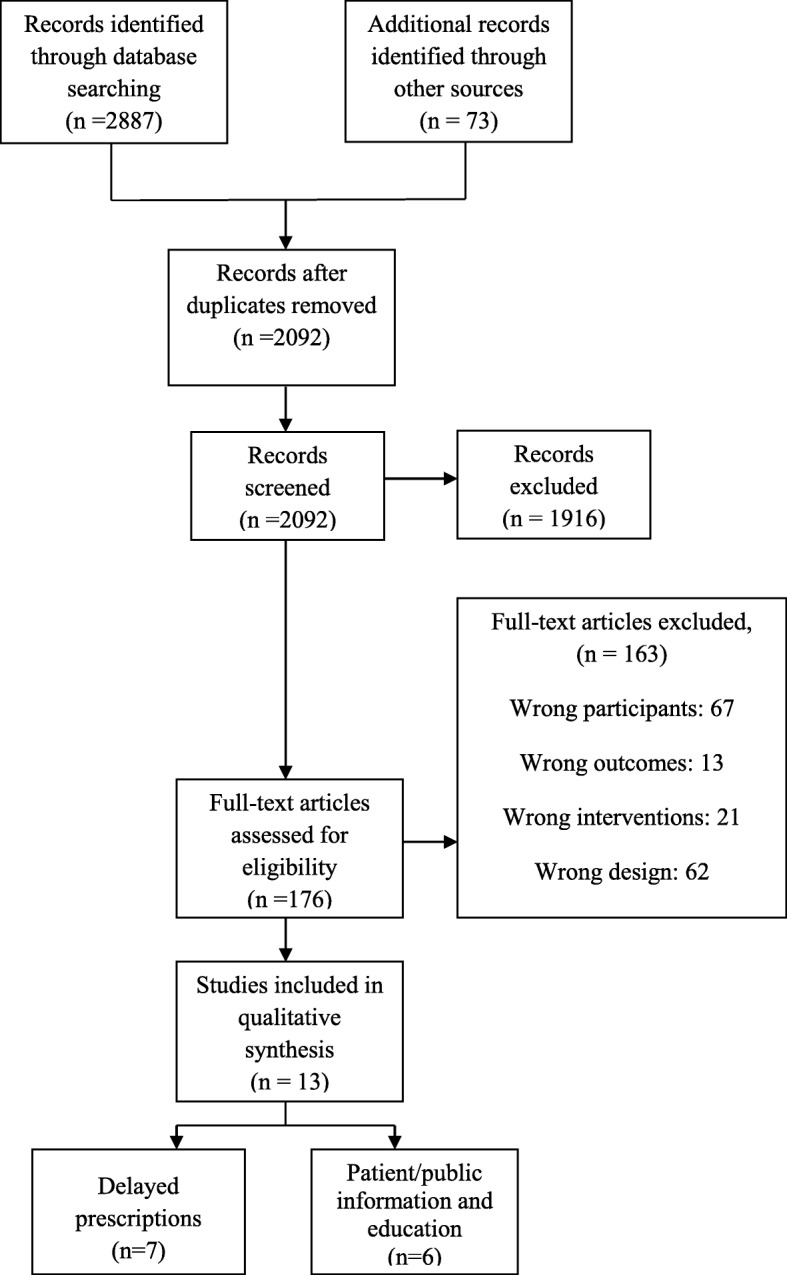
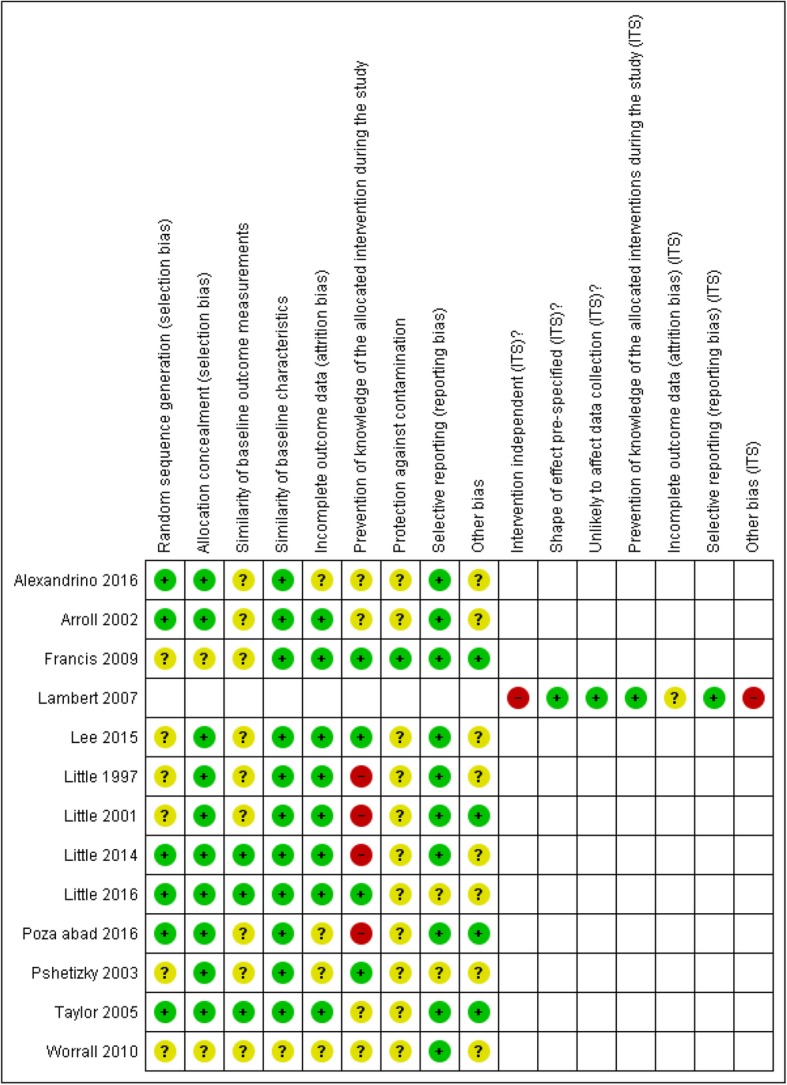
Methods: We conducted a systematic review by searching the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (OVID), EMBASE (OVID), CINAHL, and the Web of Science. We included English language randomized controlled trials (RCTs), quasi-RCTs, controlled before and after studies, and interrupted time series (ITS) studies. Two authors screened the abstract/titles and full texts, extracted data, and assessed study risk of bias. Where pooling was appropriate, a meta-analysis was performed by using a random-effects model. Where pooling of the data was not possible, a narrative synthesis of results was conducted.
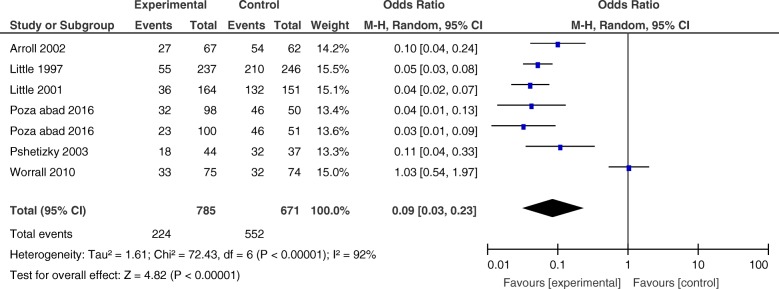
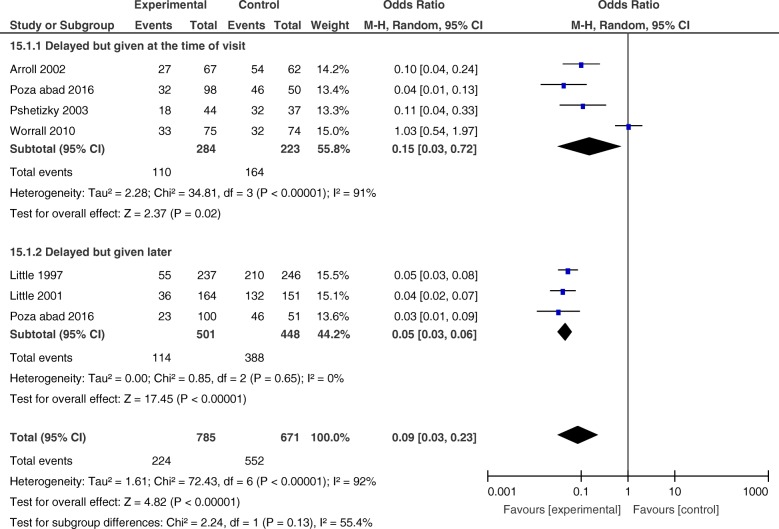
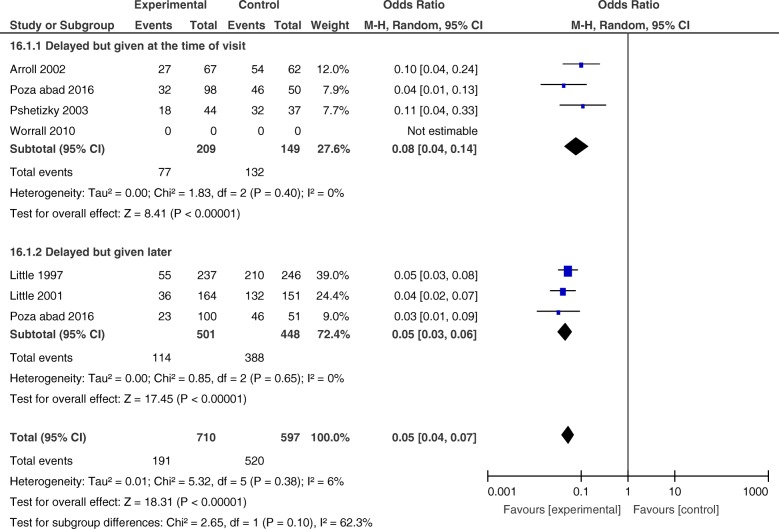
Results: We included 13 studies (one ITS, one cluster RCTs, and eleven RCTs). All interventions could be classified into two major categories: delayed prescriptions (seven studies) and patient/public information and education interventions (six studies). Our meta-analysis of delayed prescription studies observed significant reductions in the use of antibiotics for URTIs (OR = 0.09, CI 0.03 to 0.23; six studies). A subgroup analysis showed that prescriptions that were given at a later time and prescriptions that were given at the index consultation had similar effects. The studies in the patient/public information and education group varied according to their methods of delivery. Since only one or two studies were included for each method, we could not make a definite conclusion on their effectiveness. In general, booklets or pamphlets demonstrated promising effects on antibiotic prescription, if discussed by a practitioner.
Conclusions: Patient-oriented interventions (especially delayed prescriptions) may be effective in reducing antibiotic prescription for URTIs. Further research is needed to investigate the costs and feasibility of implementing these interventions as part of routine clinical practice.
Systematic review registration: PROSPERO CRD42016048007.
Keywords: Antibiotic; Delayed prescription; Meta-analysis; Patient-oriented intervention; Systematic review; Upper respiratory tract infections.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Teng CL, Tong SF, Khoo EM, Lee V, Zailinawati AH, Mimi O, et al. Antibiotics for URTI and UTI prescribing in Malaysian primary care settings. Aust Fam Physician. 2011;40(5):325–329. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
