

Levetiracetam Versus Phenobarbital for Neonatal Seizures: A Randomized Controlled Trial
- PMID: 32385134
- PMCID: PMC7263056
- DOI: 10.1542/peds.2019-3182
Levetiracetam Versus Phenobarbital for Neonatal Seizures: A Randomized Controlled Trial
Erratum in
-
Sharpe C, Reiner GE, Davis SL, et al; FOR THE NEOLEV2 INVESTIGATORS. Levetiracetam Versus Phenobarbital for Neonatal Seizures: A Randomized Controlled Trial. Pediatrics. 2020;145(6):e20193182.Pediatrics. 2021 Jan;147(1):e2020036806. doi: 10.1542/peds.2020-036806. Pediatrics. 2021. PMID: 33384298 Free PMC article. No abstract available.
Abstract
Background and objectives: There are no US Food and Drug Administration-approved therapies for neonatal seizures. Phenobarbital and phenytoin frequently fail to control seizures. There are concerns about the safety of seizure medications in the developing brain. Levetiracetam has proven efficacy and an excellent safety profile in older patients; therefore, there is great interest in its use in neonates. However, randomized studies have not been performed. Our objectives were to study the efficacy and safety of levetiracetam compared with phenobarbital as a first-line treatment of neonatal seizures.
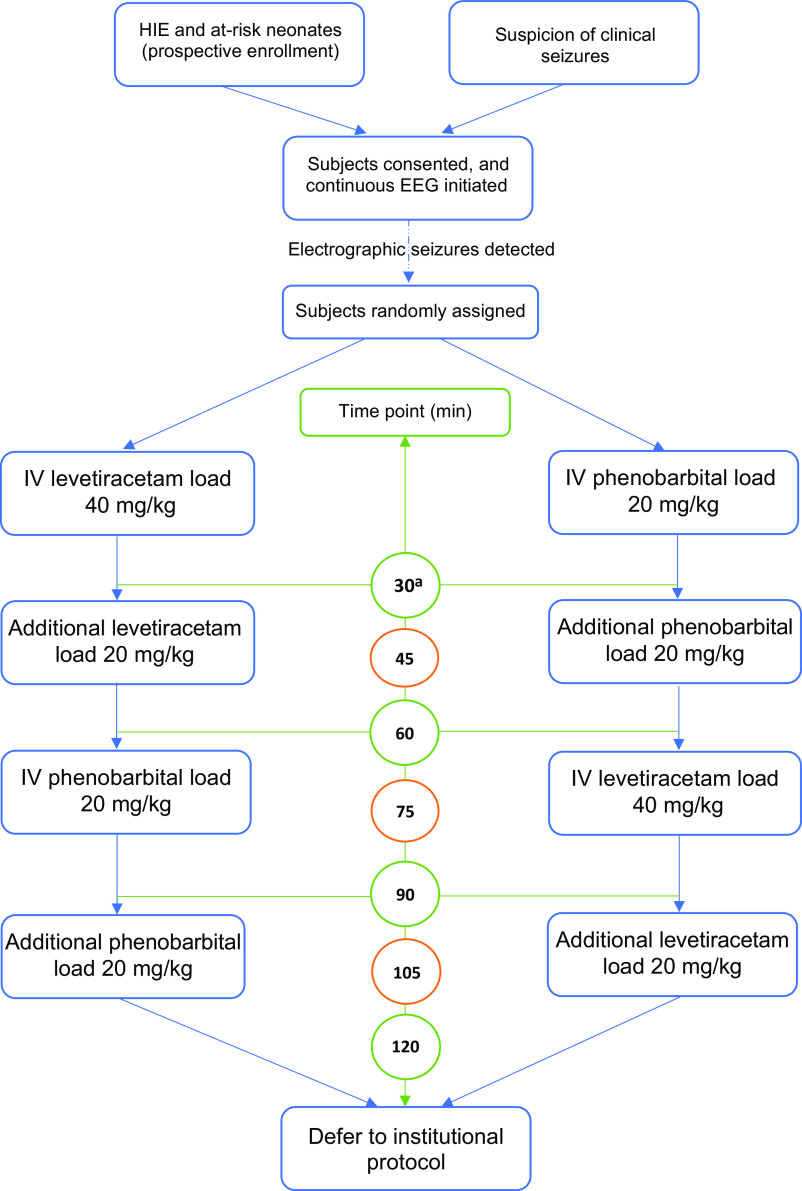
Methods: The study was a multicenter, randomized, blinded, controlled, phase IIb trial investigating the efficacy and safety of levetiracetam compared with phenobarbital as a first-line treatment for neonatal seizures of any cause. The primary outcome measure was complete seizure freedom for 24 hours, assessed by independent review of the EEGs by 2 neurophysiologists.
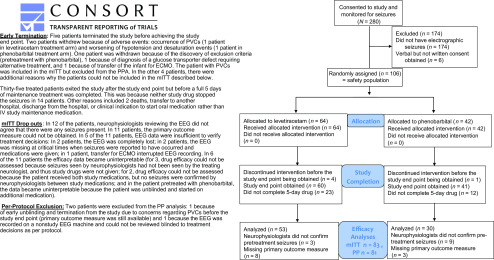
Results: Eighty percent of patients (24 of 30) randomly assigned to phenobarbital remained seizure free for 24 hours, compared with 28% of patients (15 of 53) randomly assigned to levetiracetam (P < .001; relative risk 0.35 [95% confidence interval: 0.22-0.56]; modified intention-to-treat population). A 7.5% improvement in efficacy was achieved with a dose escalation of levetiracetam from 40 to 60 mg/kg. More adverse effects were seen in subjects randomly assigned to phenobarbital (not statistically significant).
Conclusions: In this phase IIb study, phenobarbital was more effective than levetiracetam for the treatment of neonatal seizures. Higher rates of adverse effects were seen with phenobarbital treatment. Higher-dose studies of levetiracetam are warranted, and definitive studies with long-term outcome measures are needed.
Copyright © 2020 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures

References
-
- Vasudevan C, Levene M. Epidemiology and aetiology of neonatal seizures. Semin Fetal Neonatal Med. 2013;18(4):185–191 - PubMed
-
- Uria-Avellanal C, Marlow N, Rennie JM. Outcome following neonatal seizures. Semin Fetal Neonatal Med. 2013;18(4):224–232 - PubMed
-
- Holmes GL, Ben-Ari Y. Seizures in the developing brain: perhaps not so benign after all. Neuron. 1998;21(6):1231–1234 - PubMed
-
- Holmes GL. The long-term effects of neonatal seizures. Clin Perinatol. 2009;36(4):901–914, vii–viii - PubMed
-
- McBride MC, Laroia N, Guillet R. Electrographic seizures in neonates correlate with poor neurodevelopmental outcome. Neurology. 2000;55(4):506–513 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
