

Diffuse large B cell lymphoma involving Meckel's cave masquerading as biopsy-negative giant cell arteritis: a case report
- PMID: 32386515
- PMCID: PMC7211338
- DOI: 10.1186/s13256-020-02379-9
Diffuse large B cell lymphoma involving Meckel's cave masquerading as biopsy-negative giant cell arteritis: a case report
Abstract
Background: Given the absence of consensus diagnostic criteria for giant cell arteritis, clinicians may encounter difficulty with identification of new-onset headache in patients older than age 50 years presenting with visual changes and elevated inflammatory markers, particularly if temporal artery biopsies are performed and negative.
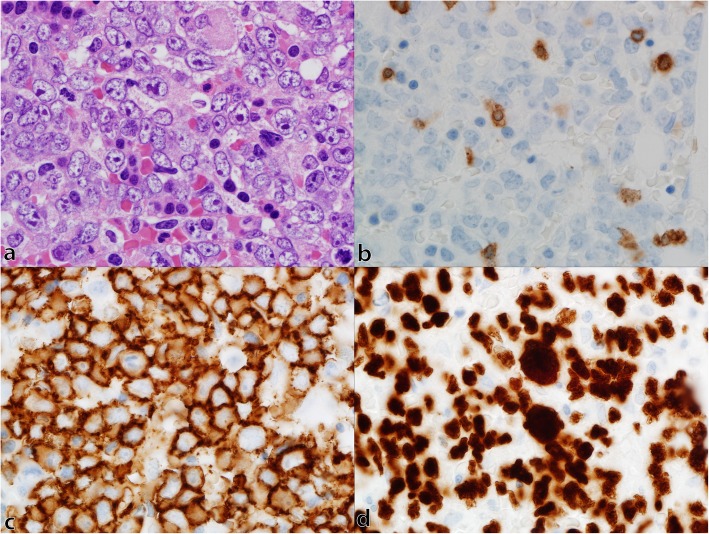
Case presentation: We present a case of a 57-year-old white man with headache, diplopia, and jaw paresthesia initially diagnosed and managed as steroid-refractory biopsy-negative giant cell arteritis. Further investigation disclosed evidence of soft tissue infiltration into Meckel's (trigeminal) cave bilaterally. Positron emission tomography suggested the presence of a lymphoproliferative disorder. Histology confirmed the diagnosis of diffuse large B cell lymphoma.
Conclusions: Metastatic involvement in Meckel's cave in diffuse large B cell lymphoma is extremely rare and presents a diagnostic challenge. Patients with suspicion of giant cell arteritis should undergo advanced imaging, particularly those with negative biopsy, atypical features, or lack of response to standard therapy, in order to assess for the presence of large-vessel vasculitis or other mimicking pathologies.
Keywords: Giant cell arteritis; Lymphoma; Metastatic; Trigeminal nerve.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Donia MM, Gamaleldin OA, Abdo AM, Desouky SE, Helmy SAS. Intracranial neoplastic lesions of the trigeminal nerve: How MRI can help. Egypt J Radiol Nucl Med. 2017;48(4):1035–1041. doi: 10.1016/j.ejrnm.2017.07.008. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
