

Tropism, replication competence, and innate immune responses of the coronavirus SARS-CoV-2 in human respiratory tract and conjunctiva: an analysis in ex-vivo and in-vitro cultures
- PMID: 32386571
- PMCID: PMC7252187
- DOI: 10.1016/S2213-2600(20)30193-4
Tropism, replication competence, and innate immune responses of the coronavirus SARS-CoV-2 in human respiratory tract and conjunctiva: an analysis in ex-vivo and in-vitro cultures
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged in December 2019, causing a respiratory disease (coronavirus disease 2019, COVID-19) of varying severity in Wuhan, China, and subsequently leading to a pandemic. The transmissibility and pathogenesis of SARS-CoV-2 remain poorly understood. We evaluate its tissue and cellular tropism in human respiratory tract, conjunctiva, and innate immune responses in comparison with other coronavirus and influenza virus to provide insights into COVID-19 pathogenesis.
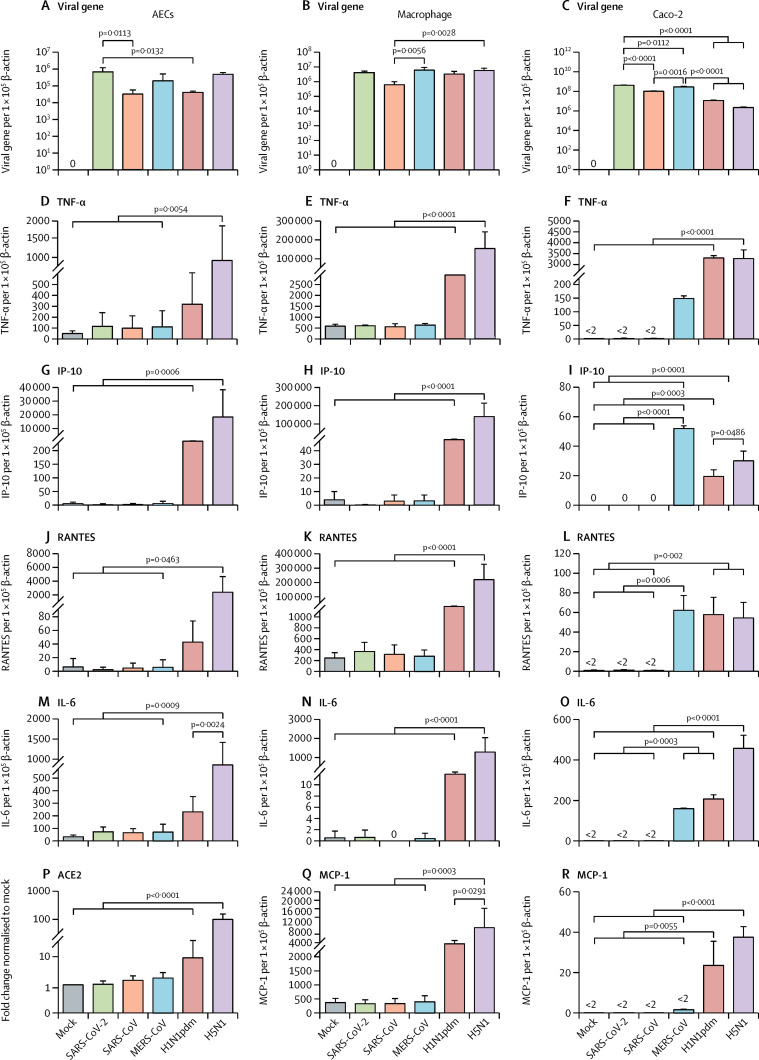
Methods: We isolated SARS-CoV-2 from a patient with confirmed COVID-19, and compared virus tropism and replication competence with SARS-CoV, Middle East respiratory syndrome-associated coronavirus (MERS-CoV), and 2009 pandemic influenza H1N1 (H1N1pdm) in ex-vivo cultures of human bronchus (n=5) and lung (n=4). We assessed extrapulmonary infection using ex-vivo cultures of human conjunctiva (n=3) and in-vitro cultures of human colorectal adenocarcinoma cell lines. Innate immune responses and angiotensin-converting enzyme 2 expression were investigated in human alveolar epithelial cells and macrophages. In-vitro studies included the highly pathogenic avian influenza H5N1 virus (H5N1) and mock-infected cells as controls.
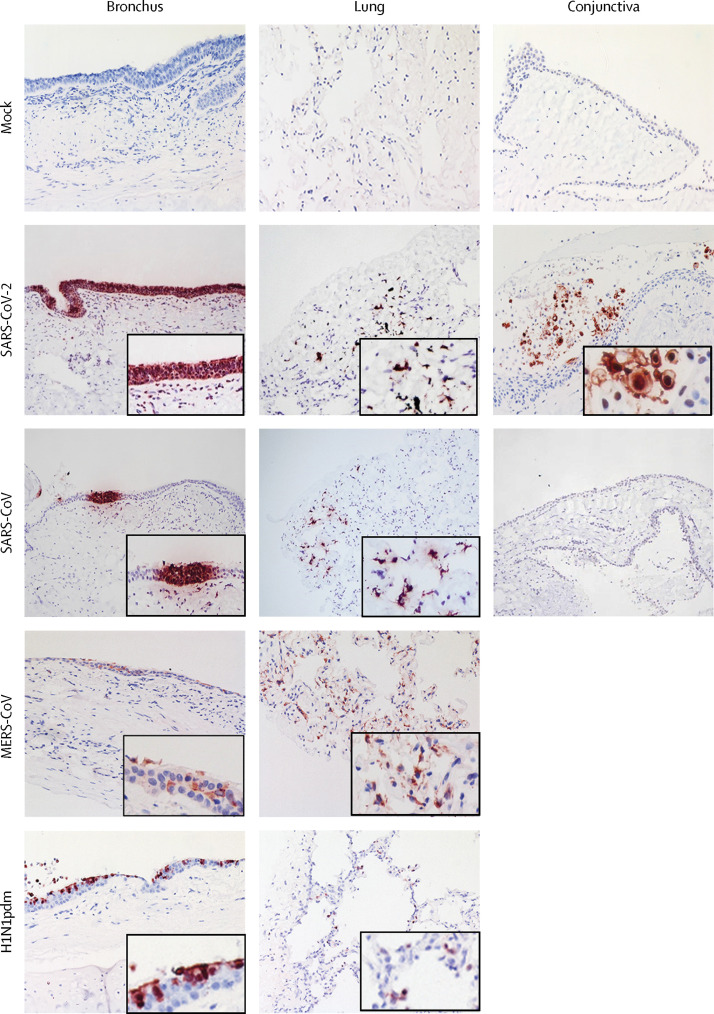
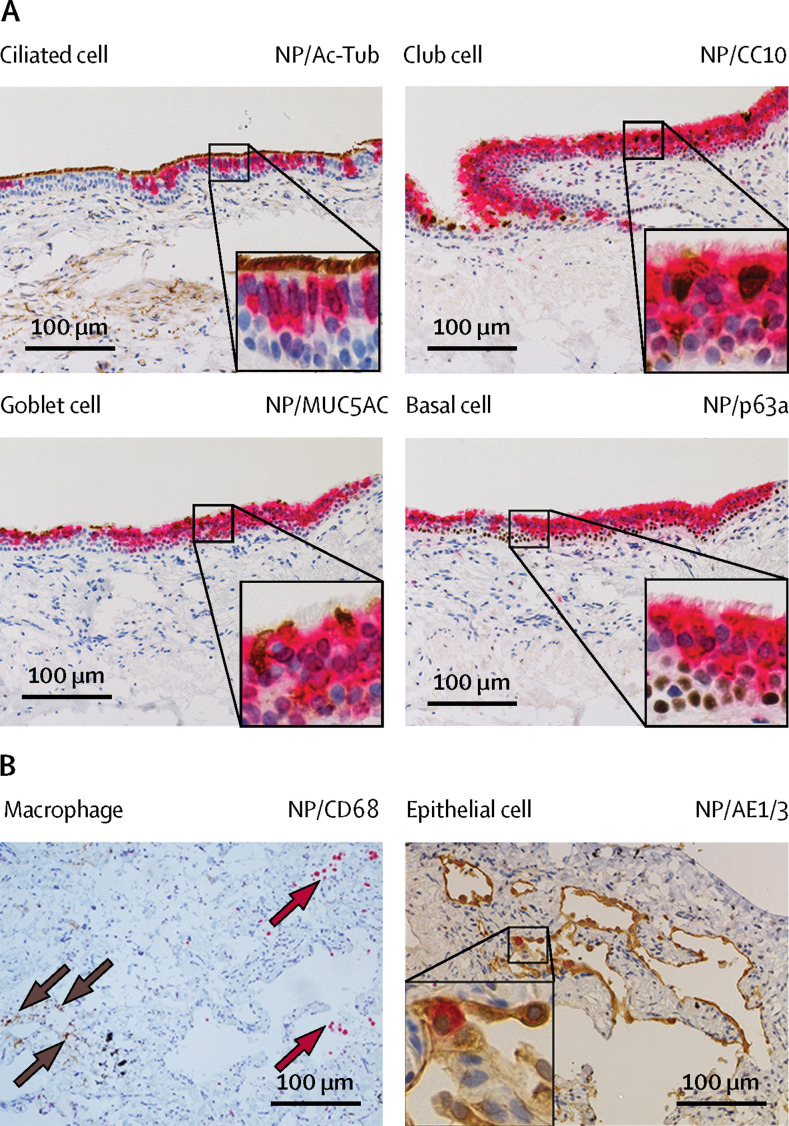
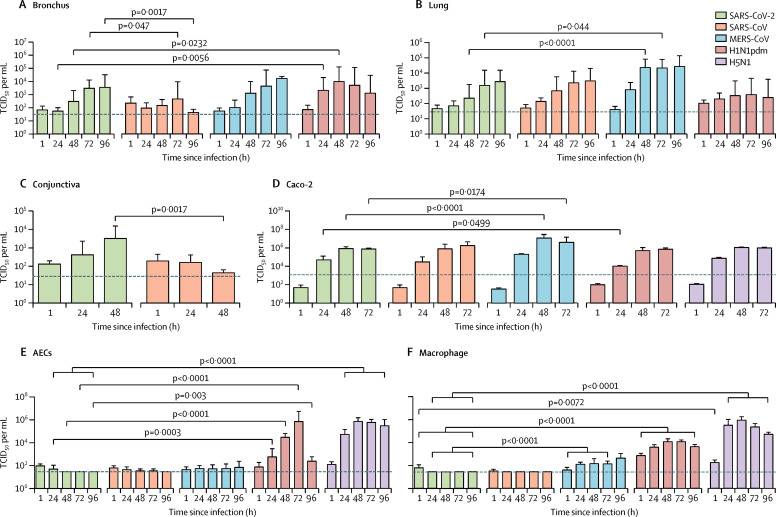
Findings: SARS-CoV-2 infected ciliated, mucus-secreting, and club cells of bronchial epithelium, type 1 pneumocytes in the lung, and the conjunctival mucosa. In the bronchus, SARS-CoV-2 replication competence was similar to MERS-CoV, and higher than SARS-CoV, but lower than H1N1pdm. In the lung, SARS-CoV-2 replication was similar to SARS-CoV and H1N1pdm, but was lower than MERS-CoV. In conjunctiva, SARS-CoV-2 replication was greater than SARS-CoV. SARS-CoV-2 was a less potent inducer of proinflammatory cytokines than H5N1, H1N1pdm, or MERS-CoV.
Interpretation: The conjunctival epithelium and conducting airways appear to be potential portals of infection for SARS-CoV-2. Both SARS-CoV and SARS-CoV-2 replicated similarly in the alveolar epithelium; SARS-CoV-2 replicated more extensively in the bronchus than SARS-CoV. These findings provide important insights into the transmissibility and pathogenesis of SARS-CoV-2 infection and differences with other respiratory pathogens.
Funding: US National Institute of Allergy and Infectious Diseases, University Grants Committee of Hong Kong Special Administrative Region, China; Health and Medical Research Fund, Food and Health Bureau, Government of Hong Kong Special Administrative Region, China.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Assessment of SARS-CoV-2 replication in the context of other respiratory viruses.Lancet Respir Med. 2020 Jul;8(7):651-652. doi: 10.1016/S2213-2600(20)30227-7. Epub 2020 May 7. Lancet Respir Med. 2020. PMID: 32386570 Free PMC article. No abstract available.
-
SARS-CoV-2 infection in conjunctival tissue.Lancet Respir Med. 2020 Jul;8(7):e57. doi: 10.1016/S2213-2600(20)30272-1. Lancet Respir Med. 2020. PMID: 32649921 Free PMC article. No abstract available.
-
SARS-CoV-2 infection in conjunctival tissue - Authors' reply.Lancet Respir Med. 2020 Jul;8(7):e58. doi: 10.1016/S2213-2600(20)30273-3. Lancet Respir Med. 2020. PMID: 32649922 Free PMC article. No abstract available.
References
-
- WHO. MERS monthly summary, November 2019. 2019 (accessed Feb 24, 2020).
-
- WHO COVID-19 dashboard. 2019. https://covid19.who.int/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
