

Renal function and coronary bypass surgery in patients with ischemic heart failure
- PMID: 32386761
- PMCID: PMC7541611
- DOI: 10.1016/j.jtcvs.2020.02.136
Renal function and coronary bypass surgery in patients with ischemic heart failure
Abstract
Objective: Chronic kidney disease is a known risk factor in cardiovascular disease, but its influence on treatment effect of bypass surgery remains unclear. We assessed the influence of chronic kidney disease on 10-year mortality and cardiovascular outcomes in patients with ischemic heart failure treated with medical therapy (medical treatment) with or without coronary artery bypass grafting.
Methods: We calculated the baseline estimated glomerular filtration rate (Chronic Kidney Disease Epidemiology Collaboration formula, chronic kidney disease stages 1-5) from 1209 patients randomized to medical treatment or coronary artery bypass grafting in the Surgical Treatment for IsChemic Heart failure trial and assessed its effect on outcome.
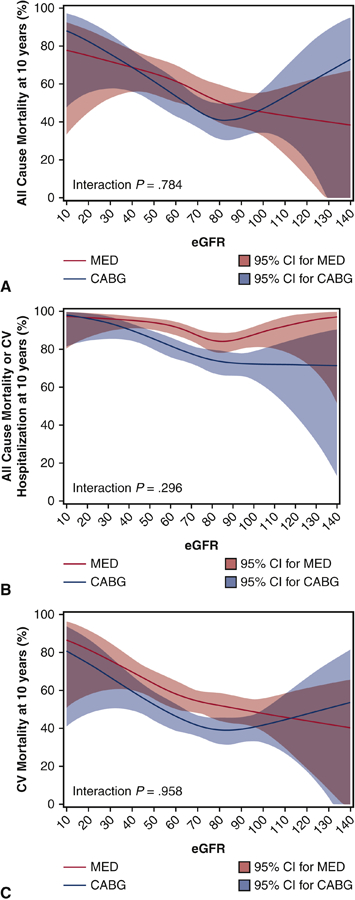
Results: In the overall Surgical Treatment for IsChemic Heart failure cohort, patients with chronic kidney disease stages 3 to 5 were older than those with stages 1 and 2 (66-71 years vs 54-59 years) and had more comorbidities. Multivariable modeling revealed an inverse association between estimated glomerular filtration rate and risk of death, cardiovascular death, or cardiovascular rehospitalization (all P < .001, but not for stroke, P = .697). Baseline characteristics of the 2 treatment arms were equal for each chronic kidney disease stage. There were significant improvements in death or cardiovascular rehospitalization with coronary artery bypass grafting (stage 1: hazard ratio, 0.71; confidence interval, 0.53-0.96, P = .02; stage 2: hazard ratio, 0.71; confidence interval, 0.59-0.84, P < .0001; stage 3: hazard ratio, 0.76; confidence interval, 0.53-0.96, P = .03). These data were inconclusive in stages 4 and 5 for insufficient patient numbers (N = 28). There was no significant interaction of estimated glomerular filtration rate with the treatment effect of coronary artery bypass grafting (P = .25 for death and P = .54 for death or cardiovascular rehospitalization).
Conclusions: Chronic kidney disease is an independent risk factor for mortality in patients with ischemic heart failure with or without coronary artery bypass grafting. However, mild to moderate chronic kidney disease does not appear to influence long-term treatment effects of coronary artery bypass grafting.
Keywords: CABG treatment effect; chronic kidney disease; coronary artery bypass grafting; medical therapy; survival.
Copyright © 2020 The American Association for Thoracic Surgery. All rights reserved.
Conflict of interest statement
Figures




Comment in
-
Commentary: Law of diminishing returns.J Thorac Cardiovasc Surg. 2022 Feb;163(2):673. doi: 10.1016/j.jtcvs.2020.02.067. Epub 2020 Feb 21. J Thorac Cardiovasc Surg. 2022. PMID: 32171487 No abstract available.
-
Commentary: Chronic kidney disease and coronary bypass surgery: Getting it right.J Thorac Cardiovasc Surg. 2022 Feb;163(2):674-675. doi: 10.1016/j.jtcvs.2020.03.051. Epub 2020 Mar 31. J Thorac Cardiovasc Surg. 2022. PMID: 32340811 No abstract available.
References
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–352. - PubMed
-
- Schefold JC, Filippatos G, Hasenfuss G, Anker SD, von Haehling S. Heart failure and kidney dysfunction: epidemiology, mechanisms and management. Nat Rev Nephrol. 2016;12:610–623. - PubMed
-
- Doenst T, Kirov H, Moschovas A, et al. Cardiac surgery 2017 reviewed. Clin Res Cardiol. 2018;107:1087–1102. - PubMed
-
- Doenst T, Wijeysundera D, Karkouti K, et al. Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2005;130:1144. - PubMed
-
- KDIGO. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney International. 2012;2.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
