

Metabolomic Markers of Kidney Function Decline in Patients With Diabetes: Evidence From the Chronic Renal Insufficiency Cohort (CRIC) Study
- PMID: 32387023
- PMCID: PMC7529642
- DOI: 10.1053/j.ajkd.2020.01.019
Metabolomic Markers of Kidney Function Decline in Patients With Diabetes: Evidence From the Chronic Renal Insufficiency Cohort (CRIC) Study
Abstract
Rationale & objective: Biomarkers that provide reliable evidence of future diabetic kidney disease (DKD) are needed to improve disease management. In a cross-sectional study, we previously identified 13 urine metabolites that had levels reduced in DKD compared with healthy controls. We evaluated associations of these 13 metabolites with future DKD progression.
Study design: Prospective cohort.
Setting & participants: 1,001 Chronic Renal Insufficiency Cohort (CRIC) participants with diabetes with estimated glomerular filtration rates (eGFRs) between 20 and 70mL/min/1.73m2 were followed up prospectively for a median of 8 (range, 2-10) years.
Predictors: 13 urine metabolites, age, race, sex, smoked more than 100 cigarettes in lifetime, body mass index, hemoglobin A1c level, blood pressure, urinary albumin, and eGFR.
Outcomes: Annual eGFR slope and time to incident kidney failure with replacement therapy (KFRT; ie, initiation of dialysis or receipt of transplant).
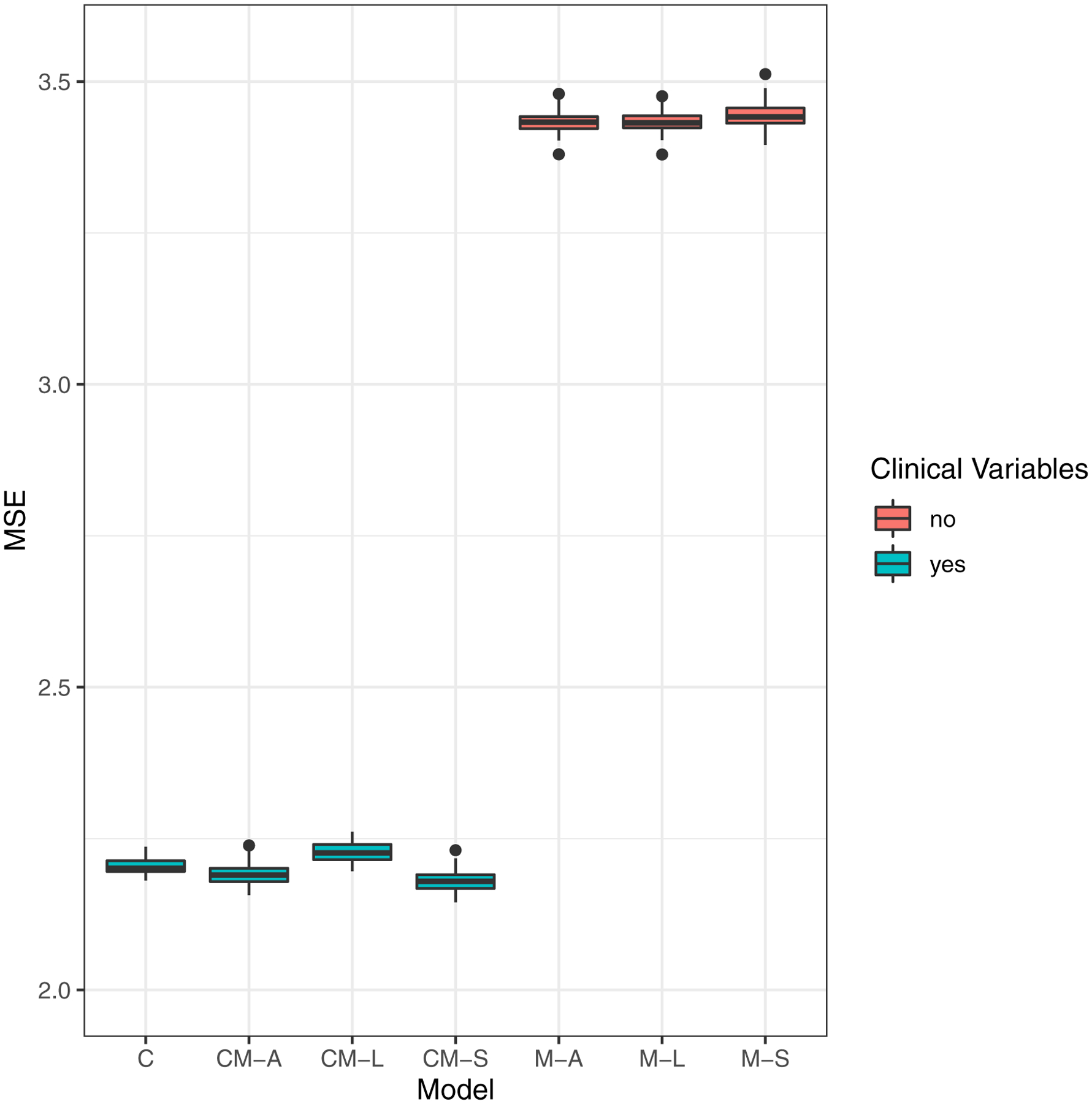
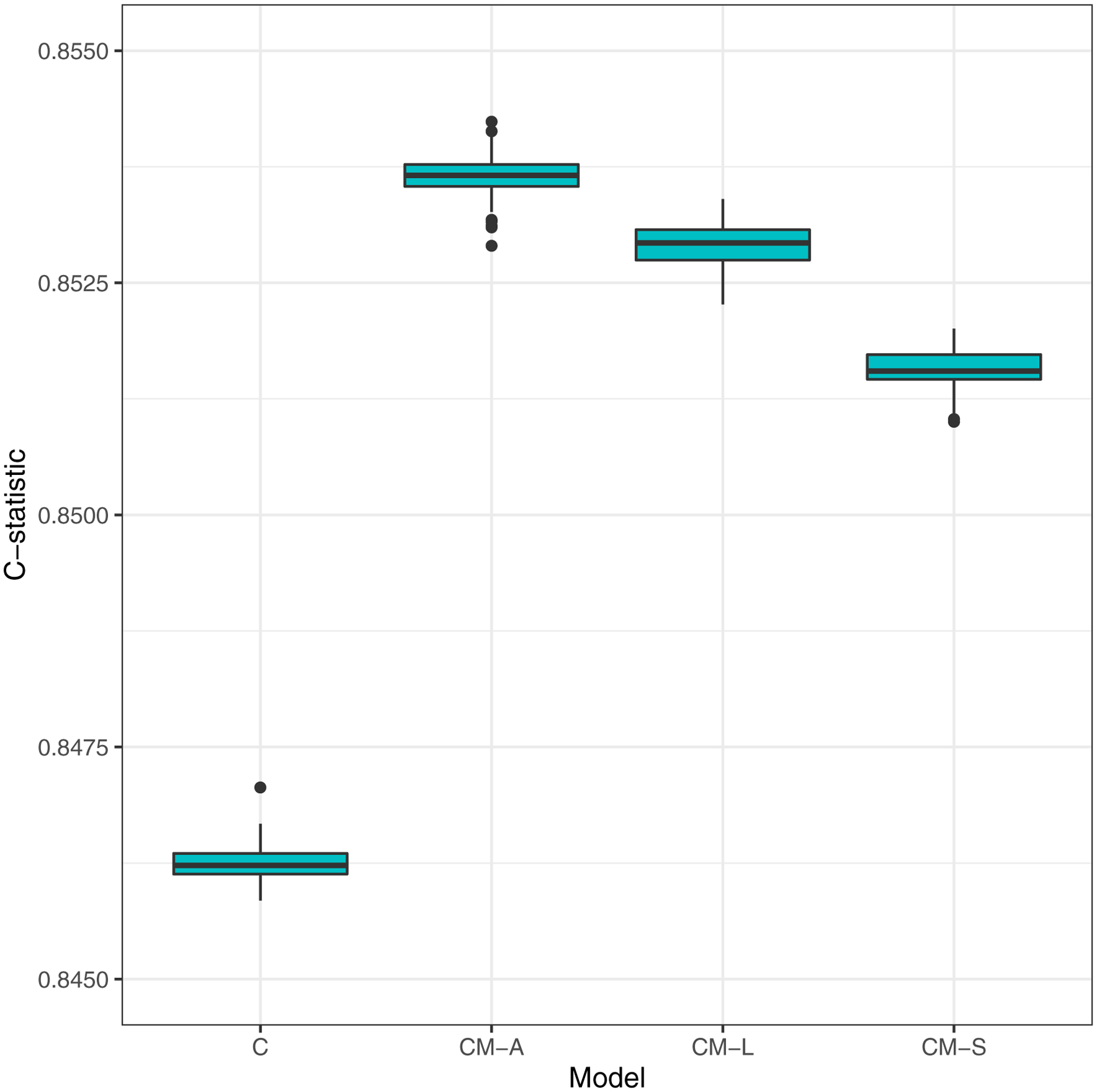
Analytical approach: Several clinical metabolite models were developed for eGFR slope as the outcome using stepwise selection and penalized regression, and further tested on the time-to-KFRT outcome. A best cross-validated (final) prognostic model was selected based on high prediction accuracy for eGFR slope and high concordance statistic for incident KFRT.
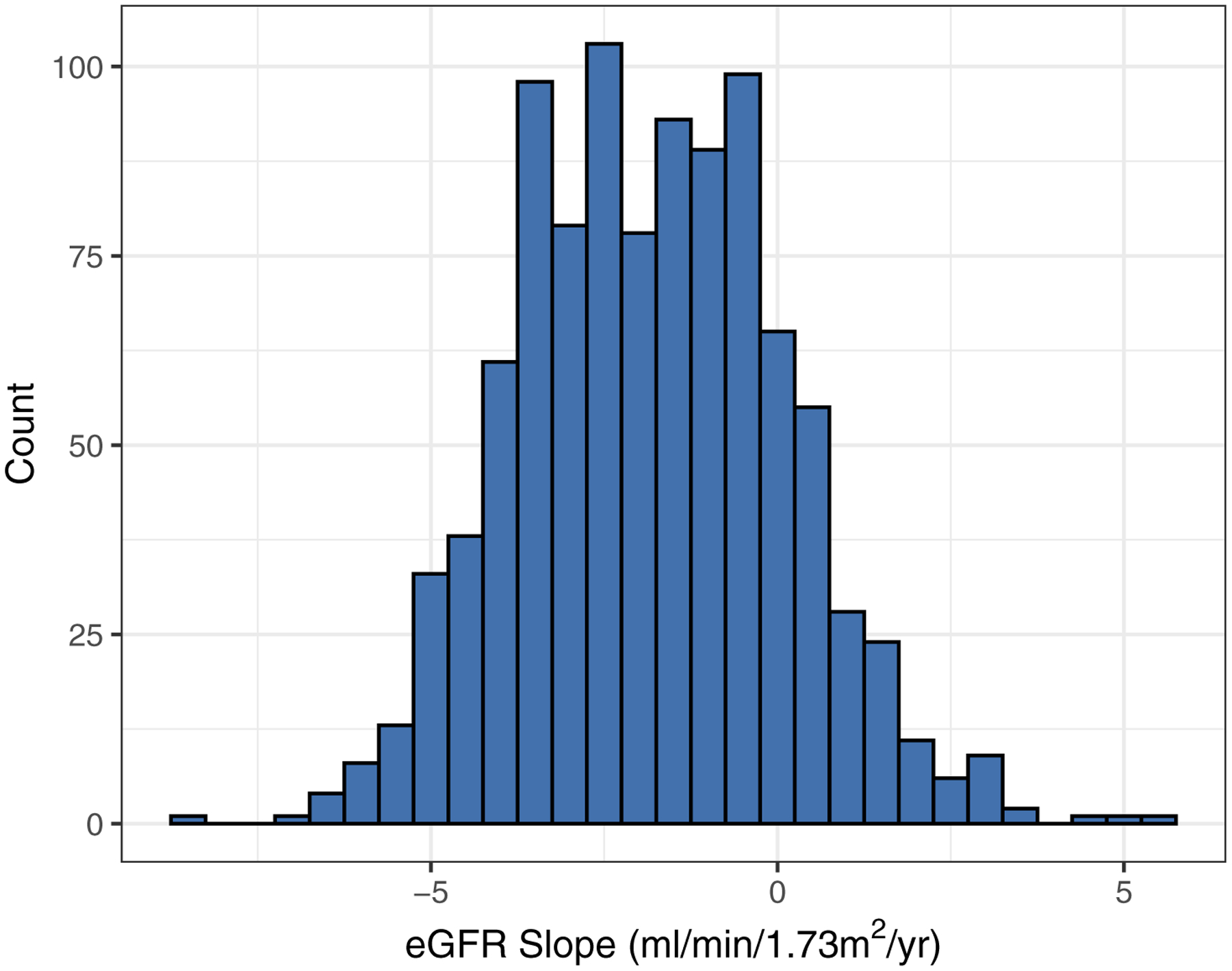
Results: During follow-up, mean eGFR slope was-1.83±1.92 (SD) mL/min/1.73m2 per year; 359 (36%) participants experienced KFRT. Median time to KFRT was 7.45 years from the time of entry to the CRIC Study. In our final model, after adjusting for clinical variables, levels of metabolites 3-hydroxyisobutyrate (3-HIBA) and 3-methylcrotonyglycine had a significant negative association with eGFR slope, whereas citric and aconitic acid were positively associated. Further, 3-HIBA and aconitic acid levels were associated with higher and lower risk for KFRT, respectively (HRs of 2.34 [95% CI, 1.51-3.62] and 0.70 [95% CI, 0.51-0.95]).
Limitations: Subgroups for whom metabolite signatures may not be optimal, nontargeted metabolomics by flow-injection analysis, and 2-stage modeling approaches.
Conclusions: Urine metabolites may offer insights into DKD progression. If replicated in future studies, aconitic acid and 3-HIBA could identify individuals with diabetes at high risk for GFR decline, potentially leading to improved clinical care and targeted therapies.
Keywords: Biomarker; Chronic Renal Insufficiency Cohort (CRIC); chronic kidney disease (CKD); diabetes; end-stage renal disease (ESRD); estimated glomerular filtration rate (eGFR); incident kidney failure; kidney disease progression; kidney function decline; longitudinal study; metabolomics; multivariate model; prediction; prognosis; risk factor.
Copyright © 2020 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK085660/DK/NIDDK NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U01 DK099924/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- R01 DK101505/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- DP3 DK094352/DK/NIDDK NIH HHS/United States
- R01 DK103784/DK/NIDDK NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U24 DK115255/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 DK104308/DK/NIDDK NIH HHS/United States
- R01 DK110541/DK/NIDDK NIH HHS/United States
- M01 RR013987/RR/NCRR NIH HHS/United States
- K23 HL125984/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- R01 HL141846/HL/NHLBI NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK099914/DK/NIDDK NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- R01 DK073665/DK/NIDDK NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- UG3 DK114915/DK/NIDDK NIH HHS/United States
- R03 HL146788/HL/NHLBI NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
