

Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management
- PMID: 32387246
- PMCID: PMC7199677
- DOI: 10.1016/j.hrthm.2020.05.001
Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management
Abstract
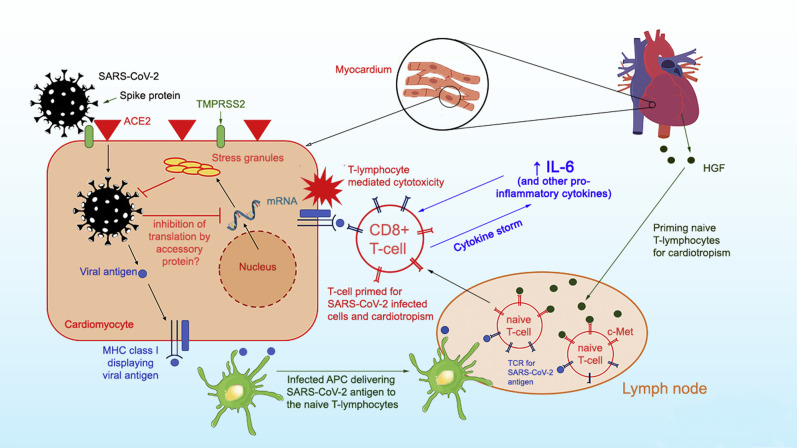
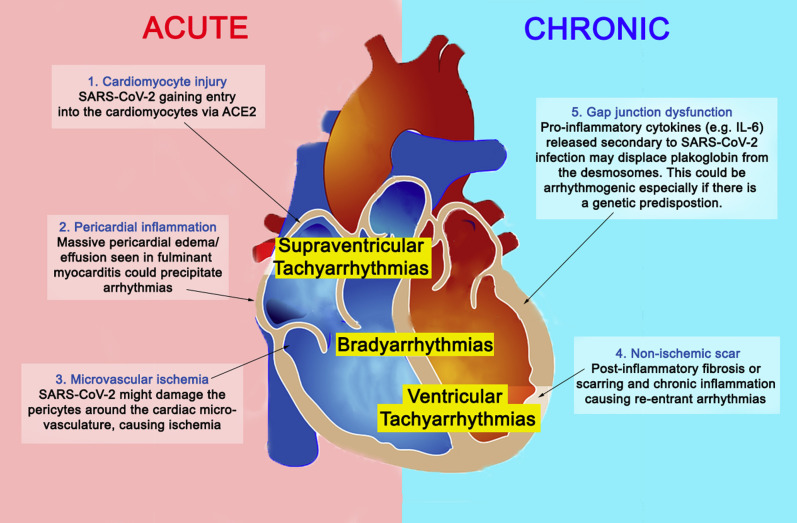
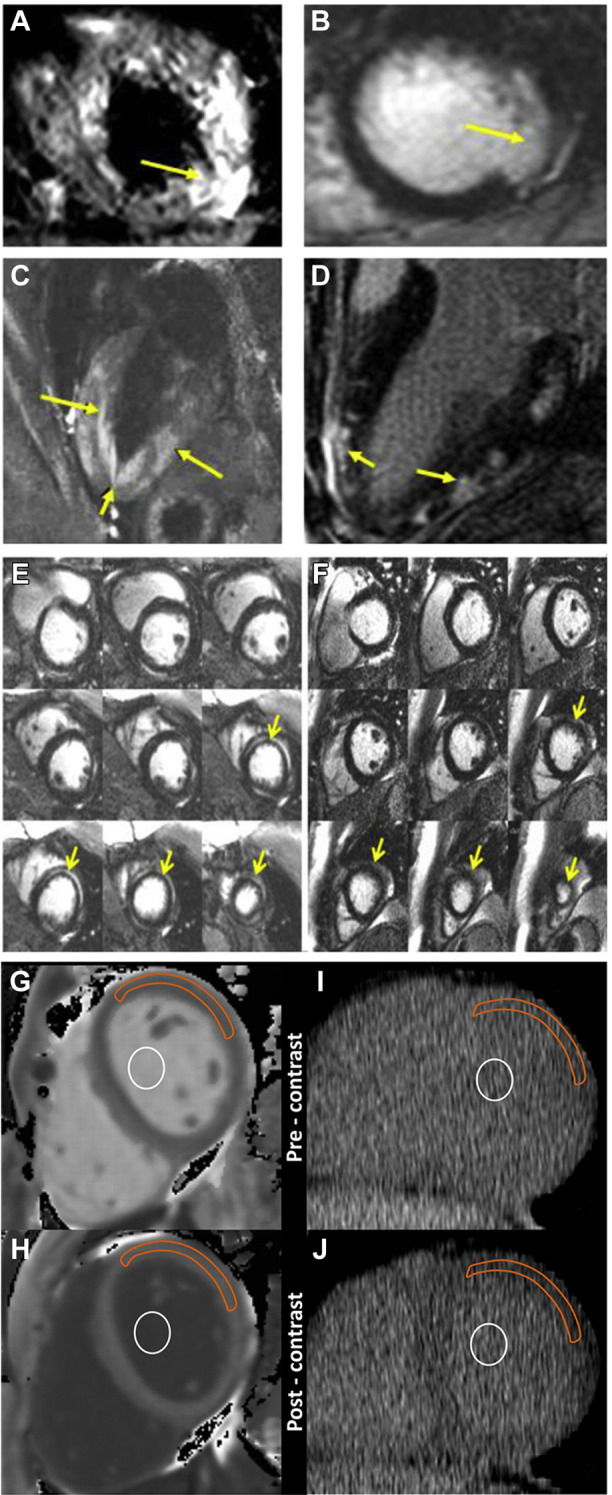
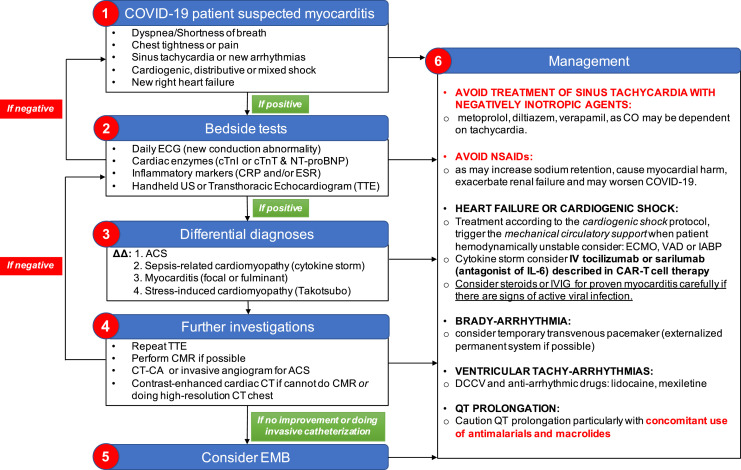
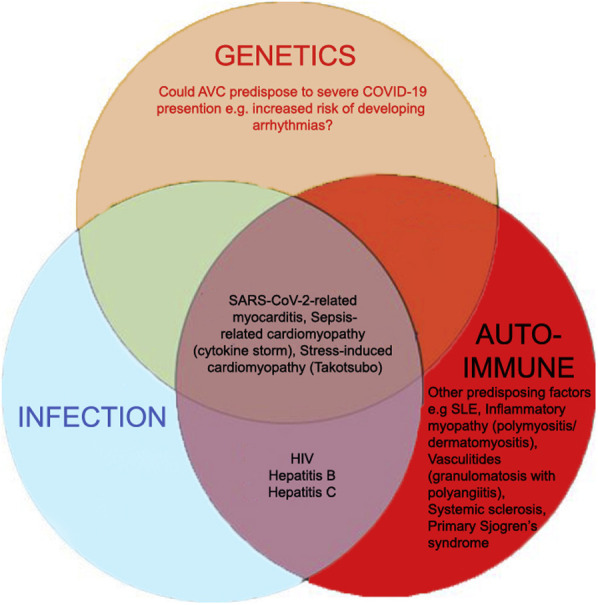
Human coronavirus-associated myocarditis is known, and a number of coronavirus disease 19 (COVID-19)-related myocarditis cases have been reported. The pathophysiology of COVID-19-related myocarditis is thought to be a combination of direct viral injury and cardiac damage due to the host's immune response. COVID-19 myocarditis diagnosis should be guided by insights from previous coronavirus and other myocarditis experience. The clinical findings include changes in electrocardiogram and cardiac biomarkers, and impaired cardiac function. When cardiac magnetic resonance imaging is not feasible, cardiac computed tomographic angiography with delayed myocardial imaging may serve to exclude significant coronary artery disease and identify myocardial inflammatory patterns. Because many COVID-19 patients have cardiovascular comorbidities, myocardial infarction should be considered. If the diagnosis remains uncertain, an endomyocardial biopsy may help identify active cardiac infection through viral genome amplification and possibly refine the treatment risks of systemic immunosuppression. Arrhythmias are not uncommon in COVID-19 patients, but the pathophysiology is still speculative. Nevertheless, clinicians should be vigilant to provide prompt monitoring and treatment. The long-term impact of COVID-19 myocarditis, including the majority of mild cases, remains unknown.
Keywords: Arrhythmias; Coronavirus disease 2019; Endomyocardial biopsy; Fulminant myocarditis; Interleukin 6; SARS-CoV-2.
Figures
References
-
- Mahase E. Covid-19: death rate is 0.66% and increases with age, study estimates. BMJ. 2020;369:m1327. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
