

Changing epidemiology and outcomes of acute kidney injury in hospitalized patients with cirrhosis - a US population-based study
- PMID: 32387698
- PMCID: PMC7994029
- DOI: 10.1016/j.jhep.2020.04.043
Changing epidemiology and outcomes of acute kidney injury in hospitalized patients with cirrhosis - a US population-based study
Abstract
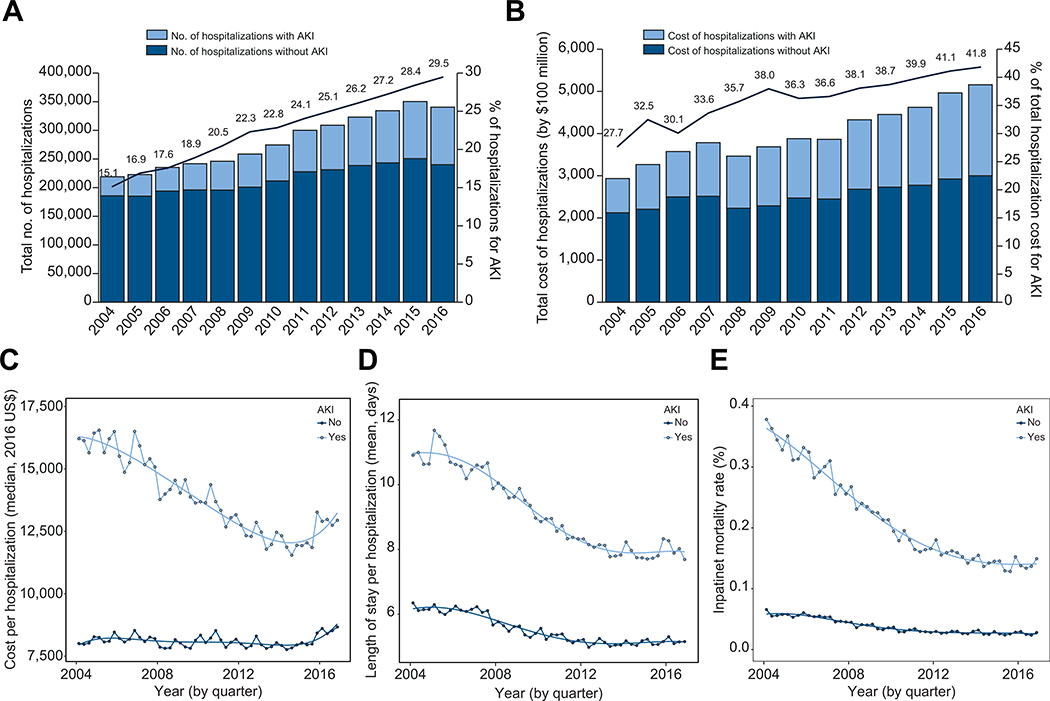
Background & aims: Acute kidney injury (AKI) is a significant clinical event in cirrhosis yet contemporary population-based studies on the impact of AKI on hospitalized cirrhotics are lacking. We aimed to characterize longitudinal trends in incidence, healthcare burden and outcomes of hospitalized cirrhotics with and without AKI using a nationally representative dataset.
Methods: Using the 2004-2016 National Inpatient Sample (NIS), admissions for cirrhosis with and without AKI were identified using ICD-9 and ICD-10 codes. Regression analysis was used to analyze the trends in hospitalizations, costs, length of stay and inpatient mortality. Descriptive statistics, simple and multivariable logistic regression were used to assess associations between individual characteristics, comorbidities, and cirrhosis complications with AKI and death.
Results: In over 3.6 million admissions for cirrhosis, 22% had AKI. AKI admissions were more costly (median $13,127 [IQR $7,367-$24,891] vs. $8,079 [IQR $4,956-$13,693]) and longer (median 6 [IQR 3-11] days vs. 4 [IQR 2-7] days). Over time, AKI prevalence doubled from 15% in 2004 to 30% in 2016. CKD was independently and strongly associated with AKI (adjusted odds ratio 3.75; 95% CI 3.72-3.77). Importantly, AKI admissions were 3.75 times more likely to result in death (adjusted odds ratio 3.75; 95% CI 3.71-3.79) and presence of AKI increased risk of mortality in key subgroups of cirrhosis, such as those with infections and portal hypertension-related complications.
Conclusions: The prevalence of AKI is significantly increased among hospitalized cirrhotics. AKI substantially increases the healthcare burden associated with cirrhosis. Despite advances in cirrhosis care, a significant gap remains in outcomes between cirrhotics with and without AKI, suggesting that AKI continues to represent a major clinical challenge.
Lay summary: Sudden damage to the kidneys is becoming more common in people who are hospitalized and have cirrhosis. Despite advances in cirrhosis care, those with damage to the kidneys remain at higher risk of dying.
Keywords: Chronic kidney disease; Cirrhosis; National inpatient sample; Portal hypertension; Renal failure.
Copyright © 2020 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflicts of interest Dr. Naga Chalasani has ongoing paid consulting activities (or had in preceding 12 months) with NuSirt, Abbvie, Afimmune (DS Biopharma), Allergan (Tobira), Madrigal, Siemens, Foresite, Galectin, Zydus, and La Jolla. These consulting activities are generally in the areas of nonalcoholic fatty liver disease and drug hepatotoxicity. Dr. Chalasani receives research grant support from Exact Sciences, Intercept, and Galectin Therapeutics where his institution receives the funding. Over the last decade, Dr. Chalasani has served as a paid consultant to more than 35 pharmaceutical companies and these outside activities have regularly been disclosed to his institutional authorities. Dr. Pere Ginès declares that he has received research funding from Mallinckrodt, Grifols and Gilead S.A. He has participated on Advisory Boards for Novartis, Promethera, Sequana, Gilead, Martin Pharmaceuticals, Ferring Pharmaceuticals and Grifols.Remaining authors have no disclosures to report. None of the aforementioned disclosures are related to the study. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology 2008;48:2064–2077. - PubMed
-
- Gines P, Schrier RW. Renal failure in cirrhosis. N Engl J Med 2009;361:1279–1290. - PubMed
-
- Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol 2015;62:968–974. - PubMed
-
- Fede G, D’Amico G, Arvaniti V, Tsochatzis E, Germani G, Georgiadis D, et al. Renal failure and cirrhosis: a systematic review of mortality and prognosis. J Hepatol 2012;56:810–818. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
