

Multi-Stage Group Testing Improves Efficiency of Large-Scale COVID-19 Screening
- PMID: 32388468
- PMCID: PMC7177109
- DOI: 10.1016/j.jcv.2020.104382
Multi-Stage Group Testing Improves Efficiency of Large-Scale COVID-19 Screening
Abstract
Background: SARS-CoV-2 test kits are in critical shortage in many countries. This limits large-scale population testing and hinders the effort to identify and isolate infected individuals.
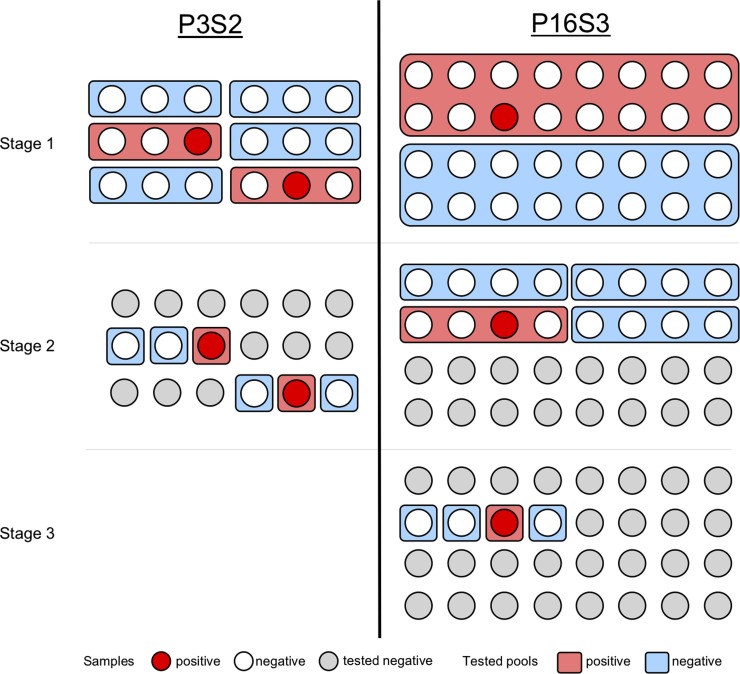
Objective: Herein, we developed and evaluated multi-stage group testing schemes that test samples in groups of various pool sizes in multiple stages. Through this approach, groups of negative samples can be eliminated with a single test, avoiding the need for individual testing and achieving considerable savings of resources.
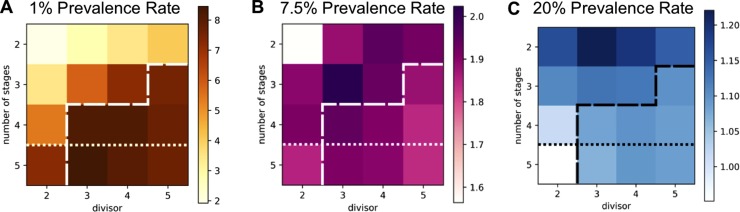
Study design: We designed and parameterized various multi-stage testing schemes and compared their efficiency at different prevalence rates using computer simulations.
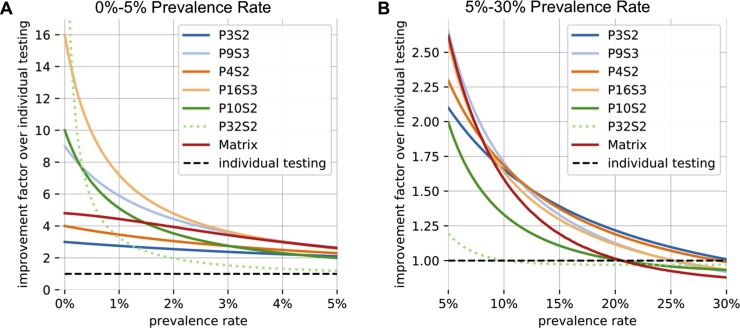
Results: We found that three-stage testing schemes with pool sizes of maximum 16 samples can test up to three and seven times as many individuals with the same number of test kits for prevalence rates of around 5% and 1%, respectively. We propose an adaptive approach, where the optimal testing scheme is selected based on the expected prevalence rate.
Conclusion: These group testing schemes could lead to a major reduction in the number of testing kits required and help improve large-scale population testing in general and in the context of the current COVID-19 pandemic.
Keywords: Group testing; Mass population tests; Testing.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
References
-
- https://www.worldometers.info/coronavirus/ (Last access: 10-14-2020).
-
- Dorfman R. The detection of defective members of large populations. Ann. Math. Stat. 1943;14(436–411)
-
- Yelin I., Aharony N., Shaer-Tamar E., Argoetti A., Messer E., Berenbaum D., Shafran E., Kuzli A., Gandali N., Hashimshony T., Mandel-Gutfreund Y., Halberthal M., Geffen Y., Szwarcwort-Cohen M., Kishony R. Evaluation of COVID-19 RT-qPCR test in multi-sample pools. medRxiv. 2020 doi: 10.1101/2020.03.26.20039438. 03.26.20039438. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
