

Role of Hyperinsulinemia and Insulin Resistance in Hypertension: Metabolic Syndrome Revisited
- PMID: 32389340
- PMCID: PMC7219403
- DOI: 10.1016/j.cjca.2020.02.066
Role of Hyperinsulinemia and Insulin Resistance in Hypertension: Metabolic Syndrome Revisited
Abstract
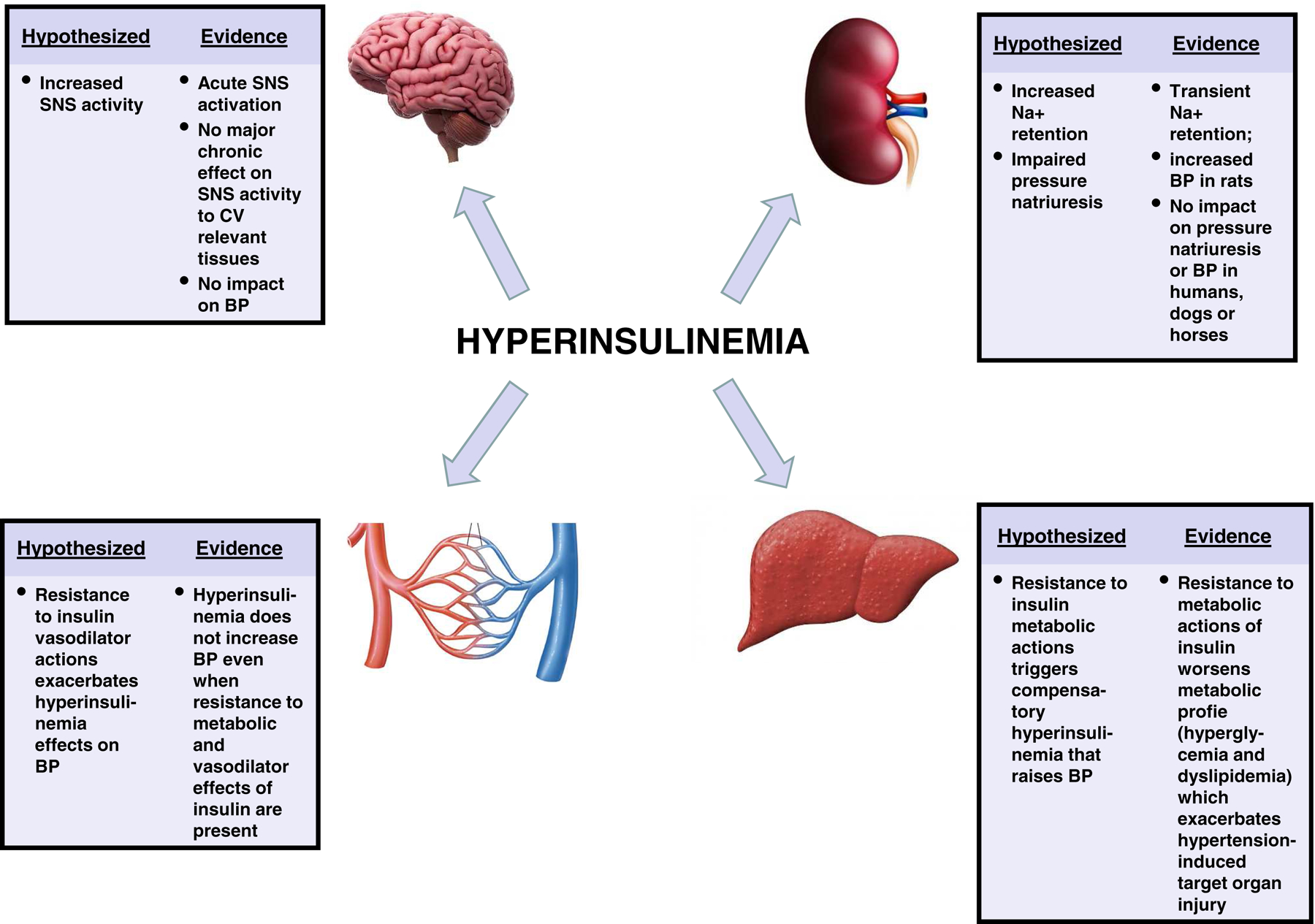
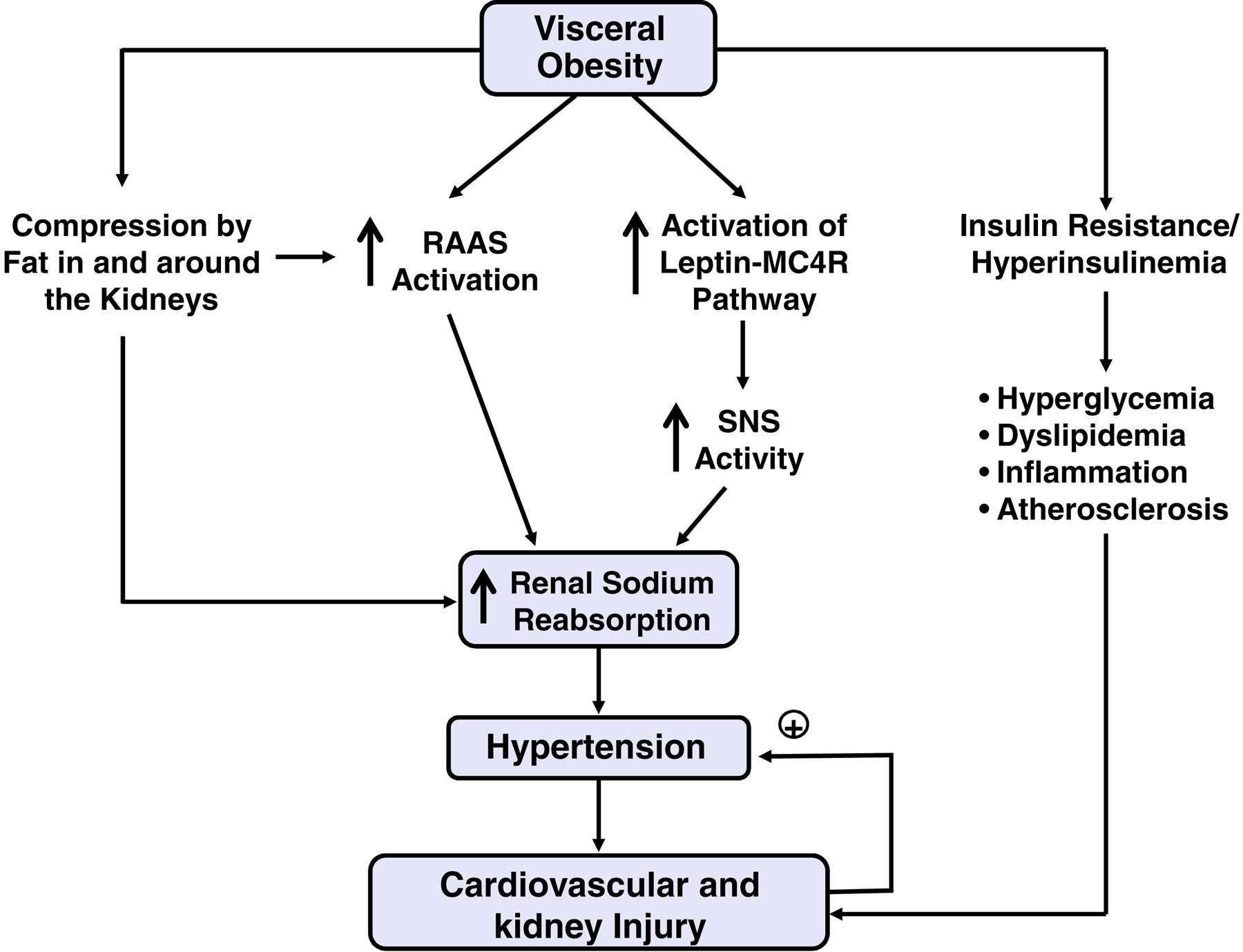
Hyperinsulinemia and insulin resistance were proposed more than 30 years ago to be important contributors to elevated blood pressure (BP) associated with obesity and the metabolic syndrome, also called syndrome X. Support for this concept initially came from clinical and population studies showing correlations among hyperinsulinemia, insulin resistance, and elevated BP in individuals with metabolic syndrome. Short-term studies in experimental animals and in humans provided additional evidence that hyperinsulinemia may evoke increases in sympathetic nervous system (SNS) activity and renal sodium retention that, if sustained, could increase BP. Although insulin infusions may increase SNS activity and modestly raise BP in rodents, chronic insulin administration does not significantly increase BP in lean or obese insulin-resistant rabbits, dogs, horses, or humans. Multiple studies in humans and experimental animals have also shown that severe insulin resistance and hyperinsulinemia may occur in the absence of elevated BP. These observations question whether insulin resistance and hyperinsulinemia are major factors linking obesity/metabolic syndrome with hypertension. Other mechanisms, such as physical compression of the kidneys, activation of the renin-angiotensin-aldosterone system, hyperleptinemia, stimulation of the brain melanocortin system, and SNS activation, appear to play a more critical role in initiating hypertension in obese subjects with metabolic syndrome. However, the metabolic effects of insulin resistance, including hyperglycemia and dyslipidemia, appear to interact synergistically with increased BP to cause vascular and kidney injury that can exacerbate the hypertension and associated injury to the kidneys and cardiovascular system.
Copyright © 2020 Canadian Cardiovascular Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
DISCLOSURES:
The authors declare no conflict of interest relevant to this manuscript.
Figures
References
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Garrison RJ, Kannel WB, Stokes J 3rd, Castelli WP. Incidence and precursors of hypertension in young adults: the Framingham Offspring Study. Prev Med. 1987;16:235–251. - PubMed
-
- Davy KP, Hall JE. Obesity and hypertension: two epidemics or one? Am J Physiol Regul Integr Comp Physiol. 2004;286:R803–813. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
