

Low-chloride- versus high-chloride-containing hypertonic solution for the treatment of subarachnoid hemorrhage-related complications: The ACETatE (A low ChloriE hyperTonic solution for brain Edema) randomized trial
- PMID: 32391156
- PMCID: PMC7197130
- DOI: 10.1186/s40560-020-00449-0
Low-chloride- versus high-chloride-containing hypertonic solution for the treatment of subarachnoid hemorrhage-related complications: The ACETatE (A low ChloriE hyperTonic solution for brain Edema) randomized trial
Erratum in
-
Correction to: Low-chloride- versus high-chloride-containing hypertonic solution for the treatment of subarachnoid hemorrhage-related complications: The ACETatE (A low ChloriE hyperTonic solution for brain Edema) randomized trial.J Intensive Care. 2020 Sep 1;8:66. doi: 10.1186/s40560-020-00485-w. eCollection 2020. J Intensive Care. 2020. PMID: 32922802 Free PMC article.
Abstract
Background: Recent reports have demonstrated that among patients with subarachnoid hemorrhage (SAH) treated with hypertonic NaCl, resultant hyperchloremia has been associated with the development of acute kidney injury (AKI). We report a trial comparing the effect of two hypertonic solutions with different chloride contents on the resultant serum chloride concentrations in SAH patients, with a primary outcome aimed at limiting chloride elevation.
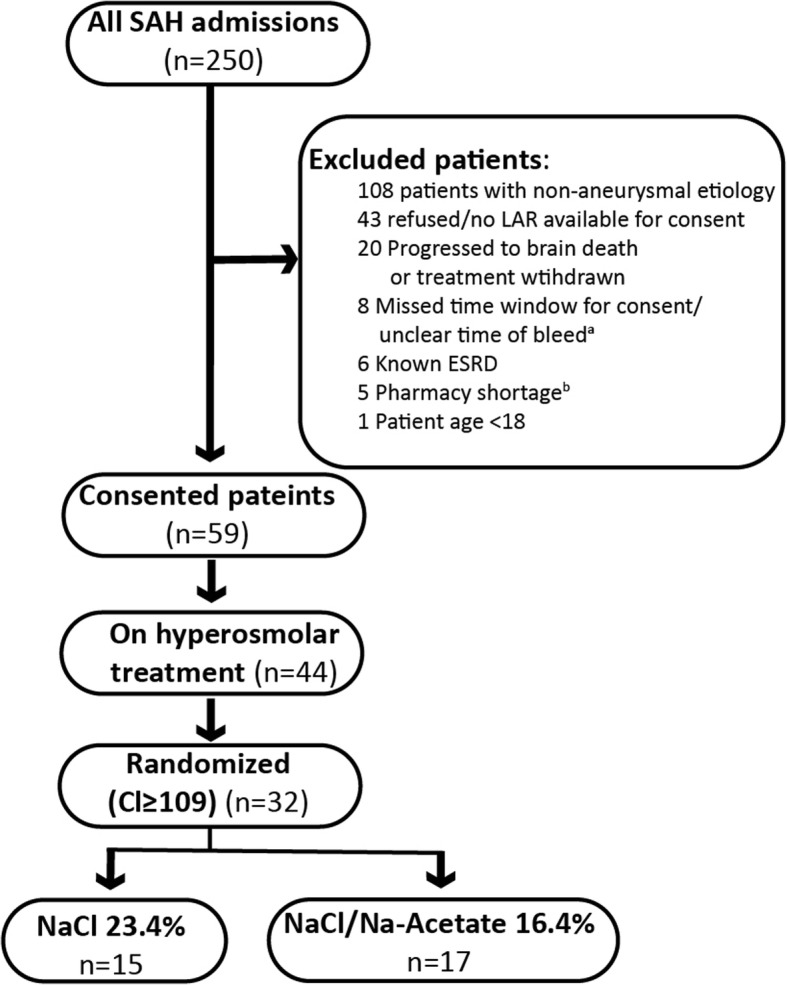
Methods: A low ChloridE hyperTonic solution for brain Edema (ACETatE) trial is a single-center, double-blinded, double-dummy, randomized pilot trial comparing bolus infusions of 23.4% NaCl and 16.4% NaCl/Na-acetate for the treatment of cerebral edema in patients with SAH. Randomization occurred when patients developed hyperchloremia (serum Cl- ≥ 109 mmol/L) and required hyperosmolar treatment.
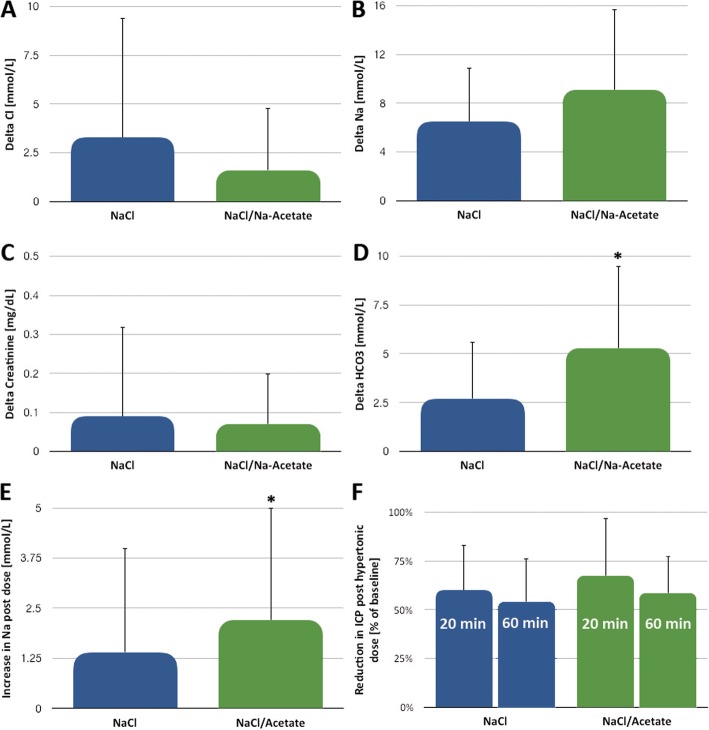
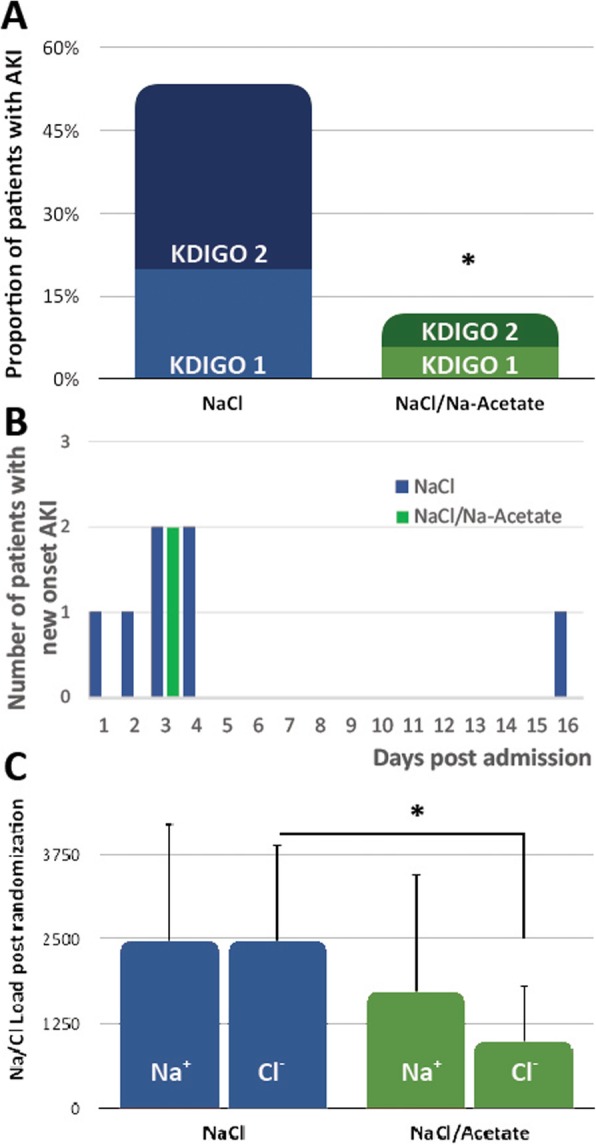
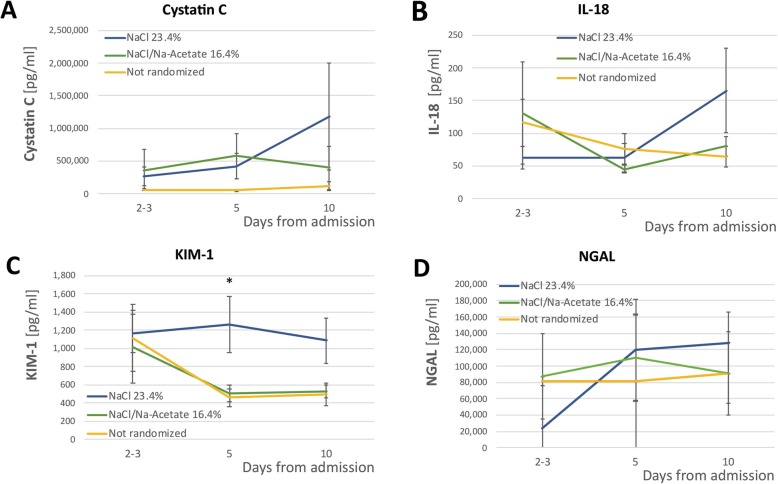
Results: We enrolled 59 patients, of which 32 developed hyperchloremia and required hyperosmolar treatment. 15 patients were randomized to the 23.4% NaCl group, and 17 patients were randomized to the 16.4% NaCl/Na-acetate group. Although serum chloride levels increased similarly in both groups, the NaCl/Acetate group showed a significantly lower Cl- load at the end of the study period (978mEq vs. 2,464mEq, p < 0.01). Secondary outcome analysis revealed a reduced rate of AKI in the Na-acetate group (53.3% in the NaCl group vs. 11.8% in the Na-acetate group, p = 0.01). Both solutions had similar effects on ICP reduction, but NaCl/Acetate treatment had a more prominent effect on immediate post-infusion Na+ concentrations (increase of 2.2 ± 2.8 vs. 1.4 ± 2.6, (p < 0.01)). Proximal tubule renal biomarkers differed in concentration between the two groups.
Conclusions: Our pilot trial showed the feasibility and safety of replacing 23.4% NaCl infusions with 16.4% NaCl/Na-acetate infusions to treat cerebral edema in patients with SAH. The degree of hyperchloremia was similar in the two groups. 16.4% NaCl/Na-acetate infusions led to lower Cl- load and AKI rates than 23.4% NaCl infusions. Further multi-center studies are needed to corroborate these results.
Trial registration: clinicaltrials.gov # NCT03204955, registered on 6/28/2017.
Keywords: Acute kidney injury; Cerebral edema; Hyperchloremia; Hyperosmolar therapy; Neurocritical care; Subarachnoid hemorrhage.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
Comment in
-
Acute kidney injury after aneurysmal subarachnoid hemorrhage: is chloride really responsible?J Intensive Care. 2020 Sep 26;8:73. doi: 10.1186/s40560-020-00492-x. eCollection 2020. J Intensive Care. 2020. PMID: 32999725 Free PMC article.
References
-
- Haley EC, Jr, Kassell NF, Torner JC, Rosenthal ES, Biswal S, Zafar SF, et al. A randomized trial of nicardipine in subarachnoid hemorrhage: angiographic and transcranial Doppler ultrasound results. A report of the Cooperative Aneurysm Study. J Neurosurg. 1993;78(4):548–553. doi: 10.3171/jns.1993.78.4.0548. - DOI - PubMed
-
- Sadan O, Singbartl K, Kandiah PA, Martin KS, Samuels OB. Hyperchloremia is associated with acute kidney injury in patients with subarachnoid hemorrhage. Crit Care Med. 2017;45(8). - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
