

Low-Dose TMP-SMX in the Treatment of Pneumocystis jirovecii Pneumonia: A Systematic Review and Meta-analysis
- PMID: 32391402
- PMCID: PMC7200085
- DOI: 10.1093/ofid/ofaa112
Low-Dose TMP-SMX in the Treatment of Pneumocystis jirovecii Pneumonia: A Systematic Review and Meta-analysis
Abstract
Background: Pneumocystis jirovecii pneumonia (PJP) remains a common and highly morbid infection for immunocompromised patients. Trimethoprim-sulfamethoxazole (TMP-SMX) is the antimicrobial treatment of choice. However, treatment with TMP-SMX can lead to significant dose-dependent renal and hematologic adverse events. Although TMP-SMX is conventionally dosed at 15-20 mg/kg/d of trimethoprim for the treatment of PJP, reduced doses may be effective and carry an improved safety profile.
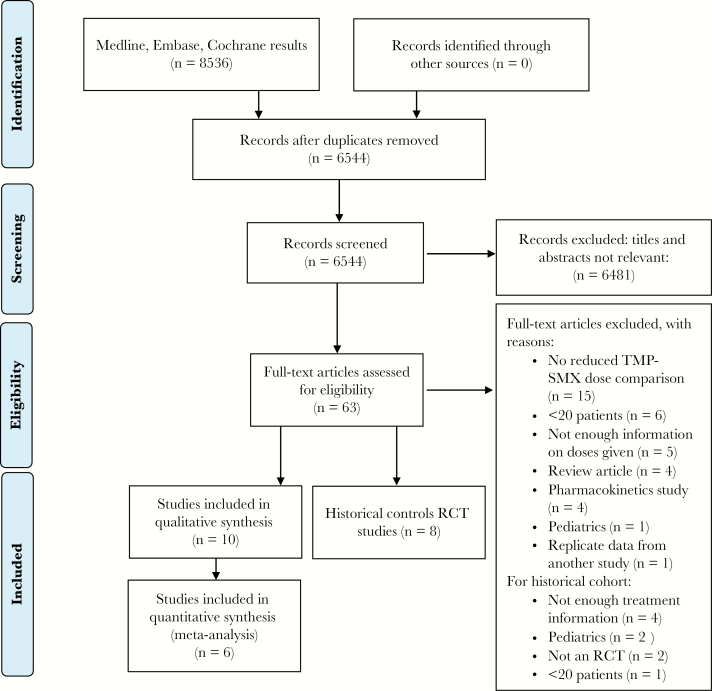
Methods: We conducted a systematic search in the Medline, Embase, and Cochrane Library databases from inception through March 2019 for peer-reviewed studies reporting on reduced doses of TMP-SMX (15 mg/kg/d of trimethoprim or less) for the treatment of PJP. PRISMA, MOOSE, and Cochrane guidelines were followed. Gray literature was excluded.
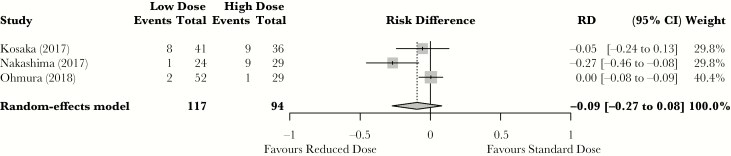
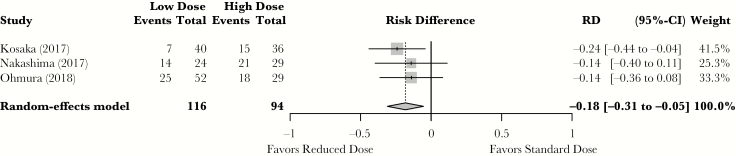
Results: Ten studies were identified, and 6 were included in the meta-analysis. When comparing standard doses with reduced doses of TMP-SMX, there was no statistically significant difference in mortality (absolute risk difference, -9% in favor of reduced dose; 95% confidence interval [CI], -27% to 8%). When compared with standard doses, reduced doses of TMP-SMX were associated with an 18% (95% CI, -31% to -5%) absolute risk reduction of grade ≥3 adverse events.
Conclusions: In this systematic review, treatment of PJP with doses of ≤10 mg/kg/d of trimethoprim was associated with similar rates of mortality when compared with standard doses and with significantly fewer treatment-emergent severe adverse events. Although limited by the observational nature of the studies included, this review provides the most current available evidence for the optimal dosing of TMP-SMX in the treatment of PJP.
Keywords: HIV; Pneumocystis jirovecii; TMP-SMX; transplantation.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Mansharamani NG, Garland R, Delaney D, Koziel H. Management and outcome patterns for adult Pneumocystis carinii pneumonia, 1985 to 1995: comparison of HIV-associated cases to other immunocompromised states. Chest 2000; 118:704–11. - PubMed
-
- Ward MM, Donald F. Pneumocystis carinii pneumonia in patients with connective tissue diseases: the role of hospital experience in diagnosis and mortality. Arthritis Rheum 1999; 42:780–9. - PubMed
-
- Medina I, Mills J, Leoung G, et al. Oral therapy for Pneumocystis carinii pneumonia in the acquired immunodeficiency syndrome. A controlled trial of trimethoprim-sulfamethoxazole versus trimethoprim-dapsone. N Engl J Med 1990; 323:776–82. - PubMed
LinkOut - more resources
Full Text Sources
Medical
