

Clinical course of severe and critical coronavirus disease 2019 in hospitalized pregnancies: a United States cohort study
- PMID: 32391519
- PMCID: PMC7205698
- DOI: 10.1016/j.ajogmf.2020.100134
Clinical course of severe and critical coronavirus disease 2019 in hospitalized pregnancies: a United States cohort study
Abstract
Background: The coronavirus disease 2019 pandemic has had an impact on healthcare systems around the world with 3 million people contracting the disease and 208,000 cases resulting in death as of this writing. Information regarding coronavirus infection in pregnancy is still limited.
Objective: This study aimed to describe the clinical course of severe and critical coronavirus disease 2019 in hospitalized pregnant women with positive laboratory testing for severe acute respiratory syndrome coronavirus 2.
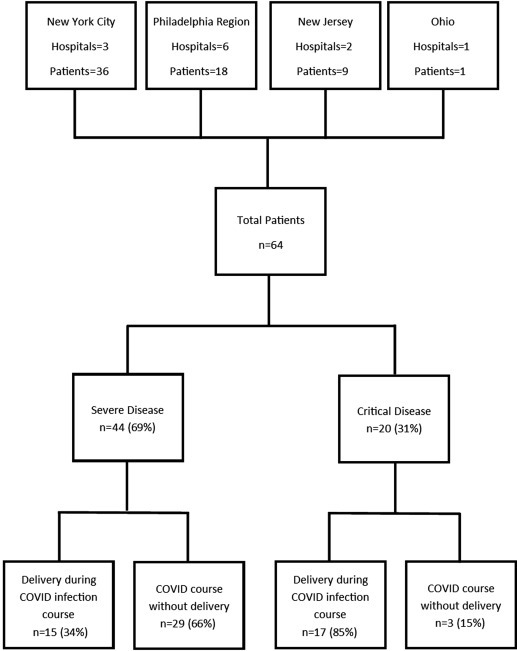
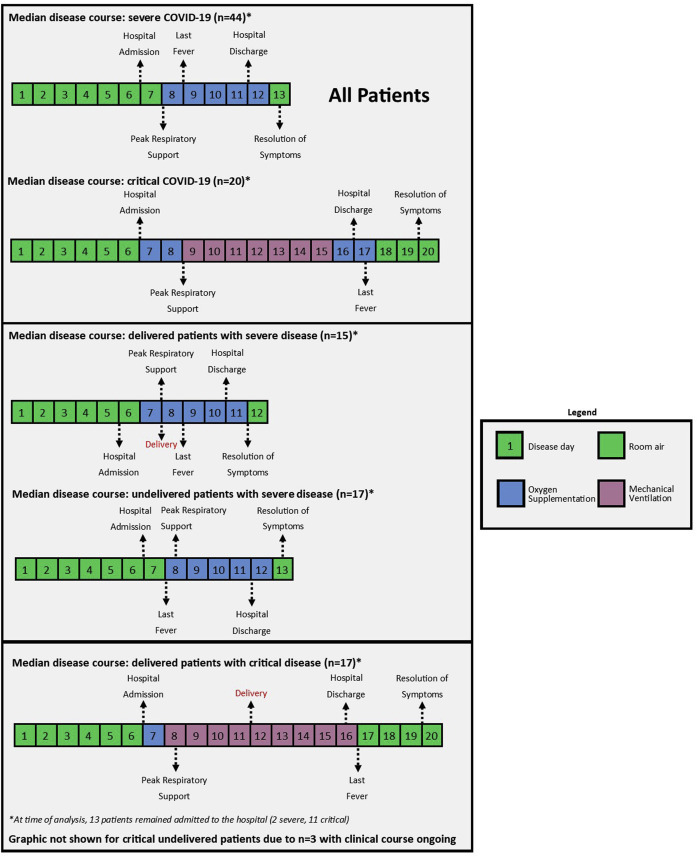
Study design: This is a cohort study of pregnant women with severe or critical coronavirus disease 2019 hospitalized at 12 US institutions between March 5, 2020, and April 20, 2020. Severe disease was defined according to published criteria as patient-reported dyspnea, respiratory rate >30 per minute, blood oxygen saturation ≤93% on room air, ratio of partial pressure of arterial oxygen to the fraction of inspired oxygen <300 mm Hg, or lung infiltrates >50% within 24-48 hours on chest imaging. Critical disease was defined as respiratory failure, septic shock, or multiple organ dysfunction or failure. Women were excluded from the study if they had presumed coronavirus disease 2019, but laboratory testing was negative. The primary outcome was median duration from hospital admission to discharge. Secondary outcomes included need for supplemental oxygen, intubation, cardiomyopathy, cardiac arrest, death, and timing of delivery. The clinical courses are described by the median disease day on which these outcomes occurred after the onset of symptoms. Treatment and neonatal outcomes are also reported.
Results: Of 64 hospitalized pregnant women with coronavirus disease 2019, 44 (69%) had severe disease, and 20 (31%) had critical disease. The following preexisting comorbidities were observed: 25% had a pulmonary condition, 17% had cardiac disease, and the mean body mass index was 34 kg/m2. Gestational age was at a mean of 29±6 weeks at symptom onset and a mean of 30±6 weeks at hospital admission, with a median disease day 7 since first symptoms. Most women (81%) were treated with hydroxychloroquine; 7% of women with severe disease and 65% of women with critical disease received remdesivir. All women with critical disease received either prophylactic or therapeutic anticoagulation during their admission. The median duration of hospital stay was 6 days (6 days [severe group] and 10.5 days [critical group]; P=.01). Intubation was usually performed around day 9 on patients who required it, and peak respiratory support for women with severe disease was performed on day 8. In women with critical disease, prone positioning was required in 20% of cases, the rate of acute respiratory distress syndrome was 70%, and reintubation was necessary in 20%. There was 1 case of maternal cardiac arrest, but there were no cases of cardiomyopathy or maternal death. Thirty-two of 64 (50%) women with coronavirus disease 2019 in this cohort delivered during their hospitalization (34% [severe group] and 85% [critical group]). Furthermore, 15 of 17 (88%) pregnant women with critical coronavirus disease 2019 delivered preterm during their disease course, with 16 of 17 (94%) pregnant women giving birth through cesarean delivery; overall, 15 of 20 (75%) women with critical disease delivered preterm. There were no stillbirths or neonatal deaths or cases of vertical transmission.
Conclusion: In pregnant women with severe or critical coronavirus disease 2019, admission into the hospital typically occurred about 7 days after symptom onset, and the duration of hospitalization was 6 days (6 [severe group] vs 12 [critical group]). Women with critical disease had a high rate of acute respiratory distress syndrome, and there was 1 case of cardiac arrest, but there were no cases of cardiomyopathy or maternal mortality. Hospitalization of pregnant women with severe or critical coronavirus disease 2019 resulted in delivery during the clinical course of the disease in 50% of this cohort, usually in the third trimester. There were no perinatal deaths in this cohort.
Keywords: COVID-19; SARS-CoV-2; coronavirus; pregnancy.
© 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- Johns Hopkins University and Medicine Coronavirus Resource Center COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) https://coronavirus.jhu.edu/map.html Available at:
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 [Epub ahead of print] - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
