

Is Recovery of Somatosensory Impairment Conditional for Upper-Limb Motor Recovery Early After Stroke?
- PMID: 32391744
- PMCID: PMC7222963
- DOI: 10.1177/1545968320907075
Is Recovery of Somatosensory Impairment Conditional for Upper-Limb Motor Recovery Early After Stroke?
Abstract
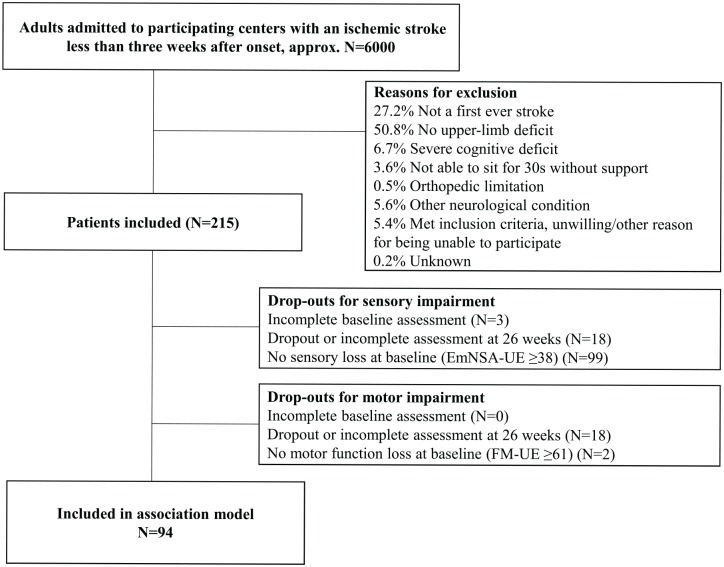
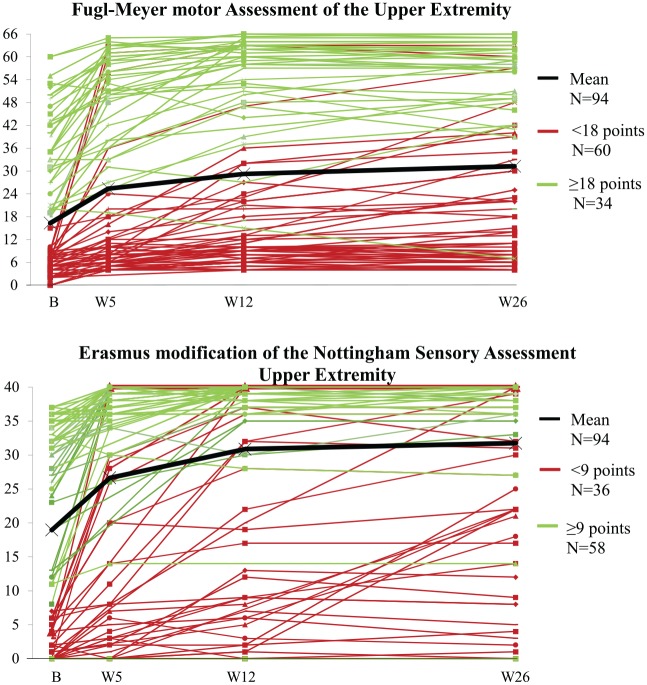
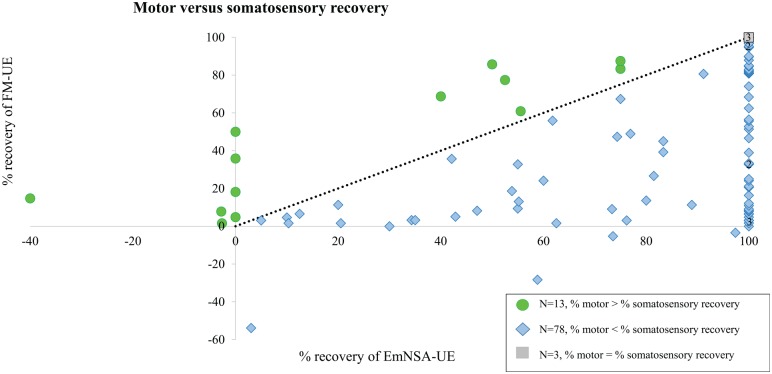
Background. Spontaneous recovery early after stroke is most evident during a time-sensitive window of heightened neuroplasticity, known as spontaneous neurobiological recovery. It is unknown whether poststroke upper-limb motor and somatosensory impairment both reflect spontaneous neurobiological recovery or if somatosensory impairment and/or recovery influences motor recovery. Methods. Motor (Fugl-Meyer upper-extremity [FM-UE]) and somatosensory impairments (Erasmus modification of the Nottingham Sensory Assessment [EmNSA-UE]) were measured in 215 patients within 3 weeks and at 5, 12, and 26 weeks after a first-ever ischemic stroke. The longitudinal association between FM-UE and EmNSA-UE was examined in patients with motor and somatosensory impairments (FM-UE ≤ 60 and EmNSA-UE ≤ 37) at baseline. Results. A total of 94 patients were included in the longitudinal analysis. EmNSA-UE increased significantly up to 12 weeks poststroke. The longitudinal association between motor and somatosensory impairment disappeared when correcting for progress of time and was not significantly different for patients with severe baseline somatosensory impairment. Patients with a FM-UE score ≥18 at 26 weeks (n = 55) showed a significant positive association between motor and somatosensory impairments, irrespective of progress of time. Conclusions. Progress of time, as a reflection of spontaneous neurobiological recovery, is an important factor that drives recovery of upper-limb motor as well as somatosensory impairments in the first 12 weeks poststroke. Severe somatosensory impairment at baseline does not directly compromise motor recovery. The study rather suggests that spontaneous recovery of somatosensory impairment is a prerequisite for full motor recovery of the upper paretic limb.
Keywords: motor activity; recovery of function; somatosensory disorders; stroke; upper extremity.
Conflict of interest statement
Figures
References
-
- Tyson SF, Hanley M, Chillala J, Selley AB, Tallis RC. Sensory loss in hospital-admitted people with stroke: characteristics, associated factors, and relationship with function. Neurorehabil Neural Repair. 2008;22:166-172. - PubMed
-
- Connell LA, Tyson SF. Measures of sensation in neurological conditions: a systematic review. Clin Rehabil. 2012;26:68-80. - PubMed
-
- Meyer S, De Bruyn N, Lafosse C, et al. Somatosensory impairments in the upper limb poststroke: distribution and association with motor function and visuospatial neglect. Neurorehabil Neural Repair. 2016;30:731-742. - PubMed
-
- Meyer S, Karttunen AH, Thijs V, Feys H, Verheyden G. How do somatosensory deficits in the arm and hand relate to upper limb impairment, activity, and participation problems after stroke? A systematic review. Phys Ther. 2014;94:1220-1232. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
