

Percutaneous vs. surgical revascularization for patients with unprotected left main stenosis: a meta-analysis of 5-year follow-up randomized controlled trials
- PMID: 32392283
- PMCID: PMC8686114
- DOI: 10.1093/ehjqcco/qcaa041
Percutaneous vs. surgical revascularization for patients with unprotected left main stenosis: a meta-analysis of 5-year follow-up randomized controlled trials
Abstract
Aims: A 5-year survival of patients with unprotected left main (ULM) stenosis according to the choice of revascularization (percutaneous vs. surgical) remains to be defined.
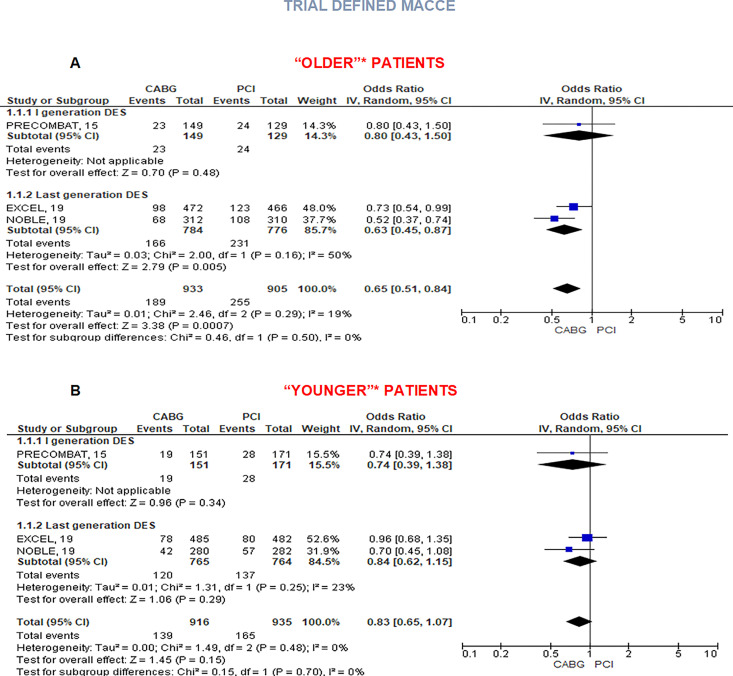
Methods and results: Randomized controlled trials (RCTs) comparing percutaneous coronary intervention (PCI) vs. coronary artery bypass graft (CABG) with a follow-up of at least 5 years were included. All-cause death was the primary endpoint. MACCE [a composite endpoint of all-cause mortality, myocardial infarction (MI), stroke, and repeat revascularization] along with its single components and cardiovascular (CV) death were the secondary ones. Analyses were stratified according to the use of first- vs. last-generation coronary stents. Subgroup comparisons were performed according to SYNTAX score (below or above 33) and to age (using cut-offs of each trial's subgroup analysis). Four RCTs with 4394 patients were identified: 2197 were treated with CABG, 657 with first generation, and 1540 with last-generation stents. At 5-year rates of all-cause death did not differ [odds ratio (OR) 0.93, 95% confidence interval (CI) 0.71-1.21], as those of CV death and stroke. Coronary artery bypass graft reduced rates of MACCE (OR 0.69, 95% CI 0.60-0.79), mainly driven by MI (OR 0.48, 95% CI 0.36-0.65) and revascularization (OR 0.53, 95% CI 0.45-0.64). Benefit of CABG for MACCE was consistent, although with different extent, across values of SYNTAX score (OR 0.76, 95% CI 0.59-0.97 for values < 32 and OR 0.63, 95% CI 0.47-0.84 for values ≥ 33) while was not evident for 'younger' patients (OR 0.83, 95% CI 0.65-1.07 vs. OR 0.65, 95% CI 0.51-0.84 for 'older' patients).
Conclusion: For patients with ULM disease followed-up for 5 years, no significant difference was observed in all-cause and cardiovascular death between PCI and CABG. Coronary artery bypass graft reduced risk of MI, revascularization, and MACCE especially in older patients and in those with complex coronary disease and a high SYNTAX score.
Keywords: Coronary artery bypass graft; Coronary artery disease; Meta-analysis; Percutaneous coronary intervention; Unprotected left main.
Published on behalf of the European Society of Cardiology.
Figures




References
-
- D'Ascenzo F, Presutti DG, Picardi E, Moretti C, Omedè P, Sciuto F et al. Prevalence and noninvasive predictors of left main or three-vessel coronary disease: evidence from a collaborative international meta-analysis including 22 740 patients. Heart 2012;98:914–919. - PubMed
-
- Yusuf S, Zucker D, Passamani E, Peduzzi P, Takaro T, Fisher LD et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists collaboration. Lancet 1994;344:563–570. - PubMed
-
- Lee PH, Ahn J-M, Chang M, Baek S, Yoon S-H, Kang S-J et al. Left main coronary artery disease: secular trends in patient characteristics, treatments, and outcomes. J Am Coll Cardiol 2016;68:1233–1246. - PubMed
-
- Palmerini T, Serruys P, Kappetein AP et al. Clinical outcomes with percutaneous coronary revascularization vs coronary artery bypass grafting surgery in patients with unprotected left main coronary artery disease: a meta-analysis of 6 randomized trials and 4,686 patients. Am Heart J 2017;190:54–63. - PubMed
-
- Head SJ, Milojevic M, Daemen J, Ahn J-M, Boersma E, Christiansen EH et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939–948. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
