

A comparison study of posterior cervical percutaneous endoscopic ventral bony decompression and simple dorsal decompression treatment in cervical spondylotic radiculopathy caused by cervical foraminal and/or lateral spinal stenosis: a clinical retrospective study
- PMID: 32393314
- PMCID: PMC7216365
- DOI: 10.1186/s12891-020-03313-2
A comparison study of posterior cervical percutaneous endoscopic ventral bony decompression and simple dorsal decompression treatment in cervical spondylotic radiculopathy caused by cervical foraminal and/or lateral spinal stenosis: a clinical retrospective study
Abstract
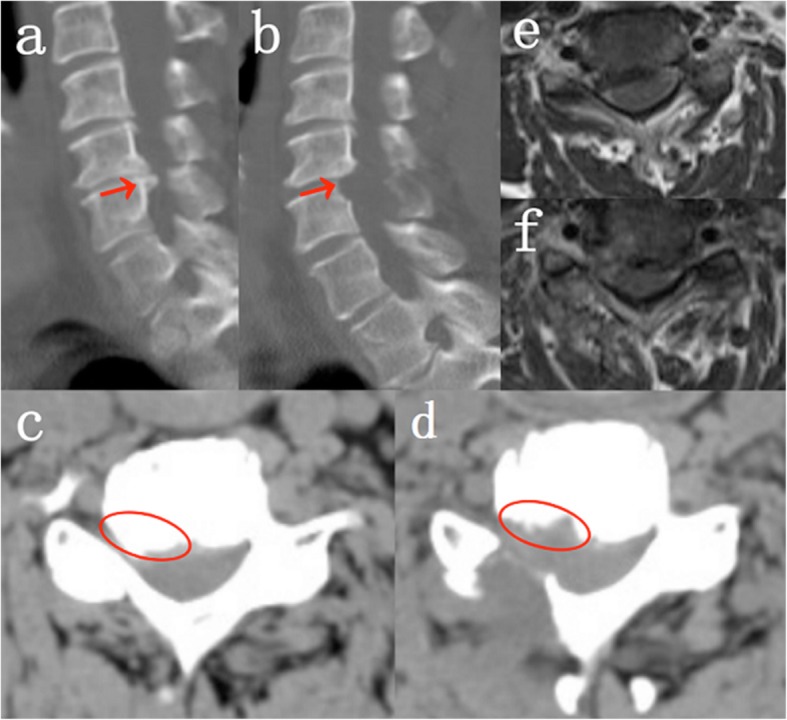
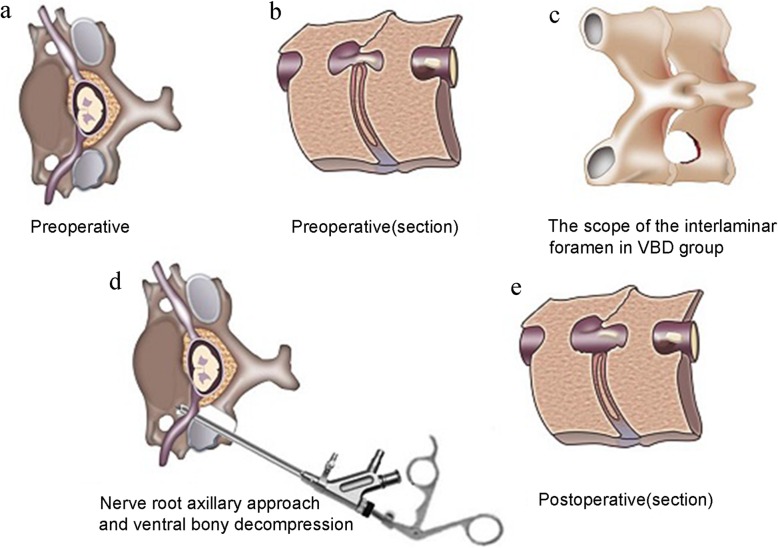
Background: Percutaneous endoscopic cervical decompression (PECD) is an ideal minimally invasive decompression technique for the treatment of cervical spondylotic radiculopathy (CSR). However, the mainstream is the resection of dorsal bone and removal of free nucleus pulposus. The necessity of excision of ventral osteophytes and hyperplastic ligaments in the treatment of CSR caused by cervical foraminal and/or lateral spinal stenosis (CFa/oLSS) to be discussed.
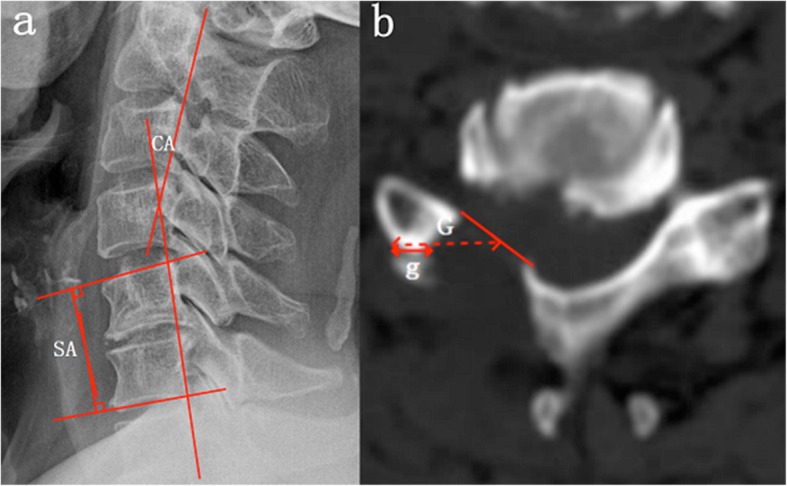
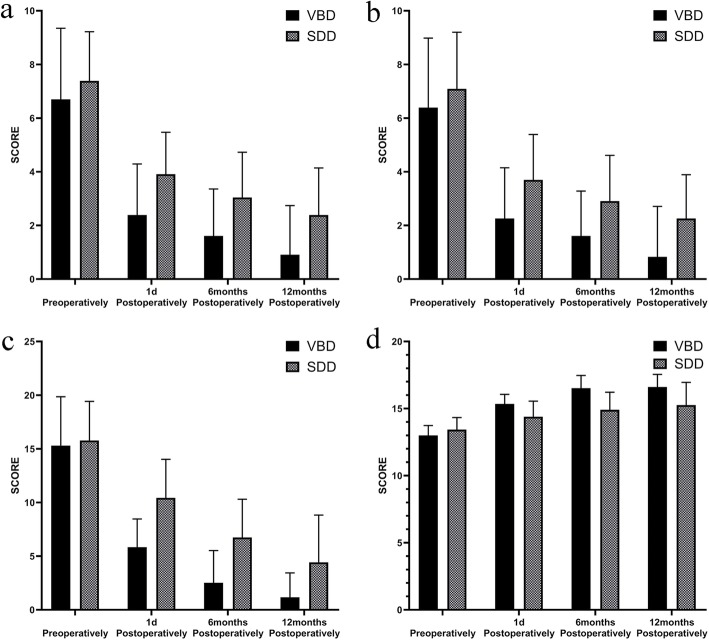
Methods: We performed a retrospective study of 46 patients with CSR caused by CFa/oLSS from January 2017 to November 2018. These patients received posterior percutaneous endoscopic cervical decompression-ventral bony decompression (PPECD-VBD)(23 cases, classified as VBD group) or posterior percutaneous endoscopic cervical decompression-simple dorsal decompression (PPECD-SDD)(23 cases, classified as SDD group). Following surgery, we recorded Visual Analogue Scale (VAS), Neck Disable Index (NDI), Japanese Orthopaedic Association (JOA) Scores and myodynamia. We further evaluated the changes of cervical curvature and cervical spine motion in the VBD group and recorded the operation time and complications during the follow-up of each patient.
Results: All patients underwent successful operations, with an average follow-up time of 16.53 ± 9.90 months. The excellent and good rates in the VBD and SDD groups were 91.29 and 60.87%, respectively. In the SDD group, neck-VAS, arm-VAS, and NDI scores were significantly higher than those of the VBD group at 1 day, 6 months, and 12 months after surgery (P < 0.05), while the JOA scores and improvement rate of JOA were significantly lower than those of the VBD group (P < 0.05). There were no significant differences in terms of angular displacement (AD), horizontal displacement (HD), segmental angle (SA) and cervical curvature (CA) before and after the operation in the VBD group (P > 0.05).
Conclusion: PPECD-VBD was significantly better than PPECD-SDD as well as PPECD-VBD had no significant effects on cervical spine stability or cervical curvature.
Keywords: Cervical foraminal and/or lateral spinal stenosis (CFa/oLSS); Cervical spondylotic radiculopathy (CSR); Minimally invasive surgery; Percutaneous endoscopic cervical decompression (PECD); Posterior percutan-eous cervical endoscopic decompression-ventral bony decompression (PPECD-VBD); Posterior percutaneous cervical endoscopic decompression-simple dorsal decompression (PPECD-SDD).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Robinson RA. Fusions of the cervical spine. J Bone Joint Surg Am. 1959;41-A(1):1–6. - PubMed
-
- Mok JK, Sheha ED, Samuel AM, McAnany SJ, Vaishnav AS, Albert TJ, Gang CH, Qureshi S. Evaluation of current trends in treatment of single-level cervical radiculopathy. Clin Spine Surg. 2019;32(5):E241–E245. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
