

Clinical impact of endemic NDM-producing Klebsiella pneumoniae in intensive care units of the national referral hospital in Jakarta, Indonesia
- PMID: 32393386
- PMCID: PMC7216366
- DOI: 10.1186/s13756-020-00716-7
Clinical impact of endemic NDM-producing Klebsiella pneumoniae in intensive care units of the national referral hospital in Jakarta, Indonesia
Abstract
Objective: A prospective observational study was performed to assess the epidemiology and clinical impact of carbapenem-non-susceptible Klebsiella pneumoniae (CNKP) in intensive care units (ICUs) of the national referral hospital in Jakarta, Indonesia.
Materials/methods: Adult patients consecutively hospitalized for > 48 h in two ICUs of the national referral hospital were included from April until October 2013 and from April until August 2014. K. pneumoniae from clinical cultures and standardized screening of rectum and throat on admission, discharge and weekly if hospitalized > 7 days were collected. Environmental niches and healthcare workers (HCWs) were also screened. Susceptibility was determined phenotypically and the presence of carbapenemase genes by PCR. Raman spectroscopy as well as multiple-locus variable number tandem repeat analysis (MLVA) were used for typing.
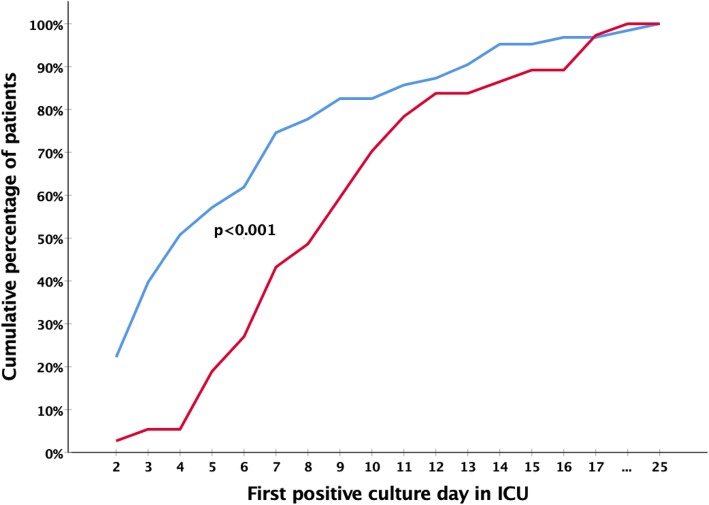
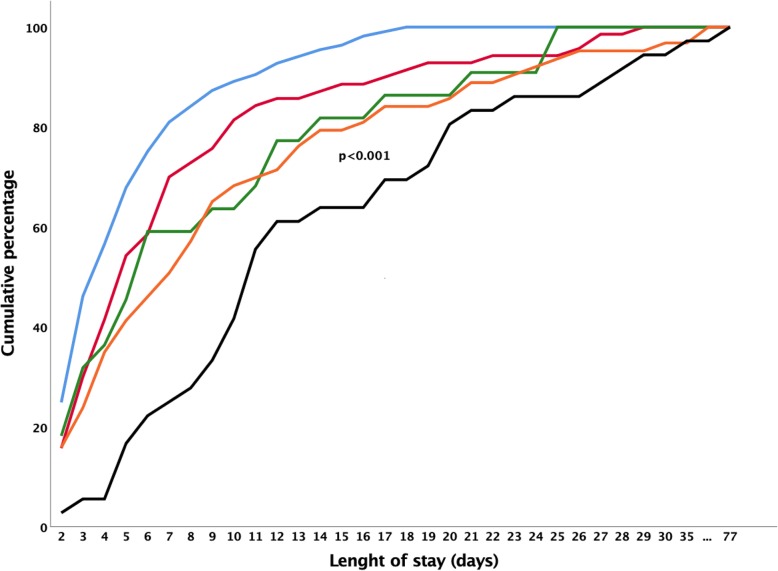
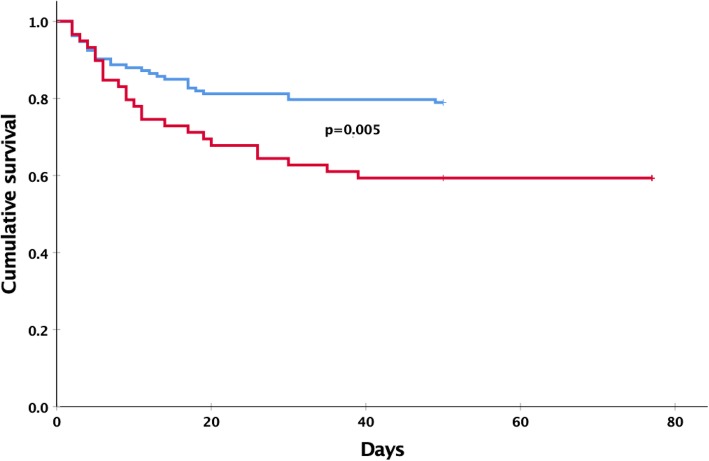
Results: Twenty-two out of 412 (5.3%) patients carried CNKP on admission and 37/390 (9.5%) acquired CNKP during ICU stay. The acquisition rate was 24.7/1000 patient-days at risk. One out of 31 (3.2%) environmental isolates was a CNKP. None of the HCWs carried CNKP. Acquisition of CNKP was associated with longer ICU stay (adjusted Hazard Ratio: 2.32 [CI99: 1.35-3.68]). ICU survival was lower among patients with CNKP compared to patients with carbapenem-susceptible K. pneumoniae (aHR 2.57, p = 0.005). Ninety-six of the 100 (96%) CNKP isolates carried a carbapenemase gene, predominantly blaNDM. Raman typing revealed three major clusters among 48 Raman types identified, whereas MLVA distinguished six major clusters among a total of 30 different genotypes.
Conclusions: NDM-producing CNKP are introduced into these ICUs and some strains expand clonally among patients and the environment, resulting in endemic CNKP. CNKP acquisition was associated with prolonged ICU stay and may affect ICU survival.
Trial registration: The study was registered at Netherlands Trial Register http://www.trialregister.nl. Candidate number: 23527, NTR number: NTR5541, NL number: NL5425 (https://www.trialregister.nl/trial/5424), Retrospectively registered: NTR: 22 December 2015.
Keywords: Carbapenemase; Indonesia; Intensive care unit; Klebsiella pneumoniae; Microbial drug resistance; Mortality.
Conflict of interest statement
YRS is an awardee of the DIKTI-NESO Scholarship by The Directorate General of Higher Education of Indonesia Ministry of Research, Technology and Higher Education of the Republic of Indonesia, and Department of Medical Microbiology and Infectious Diseases, Erasmus MC in Rotterdam, The Netherlands.
All authors report no conflict of interest relevant to this article.
Figures


References
-
- Tängdén T, Giske CG. Global dissemination of extensively drug-resistant carbapenemase-producing Enterobacteriaceae: clinical perspectives on detection, treatment and infection control. J Intern Med. 2015;277(5):501–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
