

Endovascular treatment for aortic arch pathologies: chimney, on-the-table fenestration, and in-situ fenestration techniques
- PMID: 32395281
- PMCID: PMC7212147
- DOI: 10.21037/jtd.2020.03.10
Endovascular treatment for aortic arch pathologies: chimney, on-the-table fenestration, and in-situ fenestration techniques
Abstract
Background: Revascularization of the supra-aortic major branches in thoracic endovascular aortic repair (TEVAR) is challenging owing to the complex anatomic configuration of aortic arch pathologies. This study aims to evaluate the feasibility, effectiveness, and safety of three major techniques-chimney, fenestrated, and in-situ fenestration-for patients with aortic arch pathologies.
Methods: A retrospective analysis was performed involving 234 patients with aortic arch lesions, who underwent TEVAR with adaptations in technique (chimney, fenestrated, or in-situ fenestration) between January 2016 and December 2017.
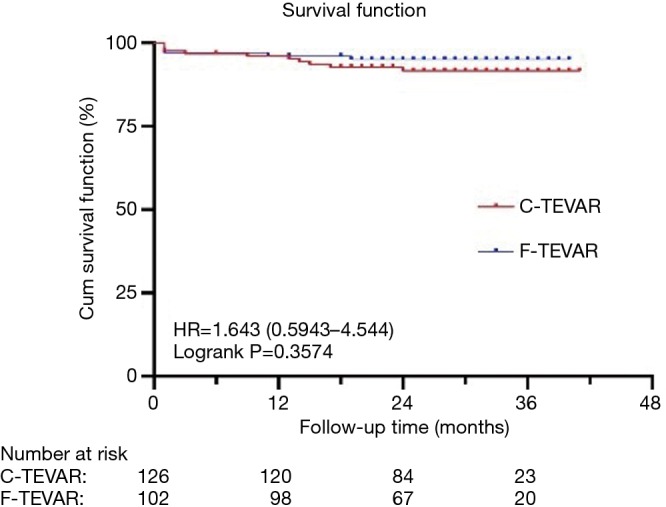
Results: One hundred and twenty-six patients underwent the chimney technique (98 single chimneys, 24 double chimneys, and four triple chimneys); one hundred and two patients (102/234) were treated with on-the-table fenestration technique (92 single fenestrations, nine double fenestrations, and one double fenestration plus innominate artery chimney); and the remaining six patients underwent in-situ needle fenestration technique. Overall, indications included aortic dissections (99/234), aortic arch aneurysms (60/234), penetrating aortic ulcers (72/234), and re-interventions (3/234). The technical success rates were 99.6%. There were five cases of early all-cause mortality. The patency rates of overall branches were 99.6%. There were 15 cases with type Ia endoleak-14 in the chimney group (11.1%) and one in the on-the-table fenestration group (1%). Five patients underwent re-interventions. The median follow-up time for all patients was 28 (range, 16-41) months.
Conclusions: Our experience suggests that chimney, on-the-table fenestration, and in-situ needle fenestration techniques are feasible, effective, and safe treatment options for aortic arch pathologies with encouraging mid-term results. Long-term durability concerns require further evaluation.
Keywords: Endovascular procedure; aneurysm; aortic diseases; dissecting.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources
Medical