

Effects of non-invasive ventilation in subjects undergoing cardiac surgery on length of hospital stay and cardiac-pulmonary complications: a systematic review and meta-analysis
- PMID: 32395288
- PMCID: PMC7212120
- DOI: 10.21037/jtd.2020.02.30
Effects of non-invasive ventilation in subjects undergoing cardiac surgery on length of hospital stay and cardiac-pulmonary complications: a systematic review and meta-analysis
Abstract
Background: Cardiac surgery often leads to pulmonary complications. Non-invasive ventilation (NIV) is a mechanical ventilation modality that may help to prevent the pulmonary complications, and the role of the prophylactic use of NIV in patients after cardiac surgery remains controversial.
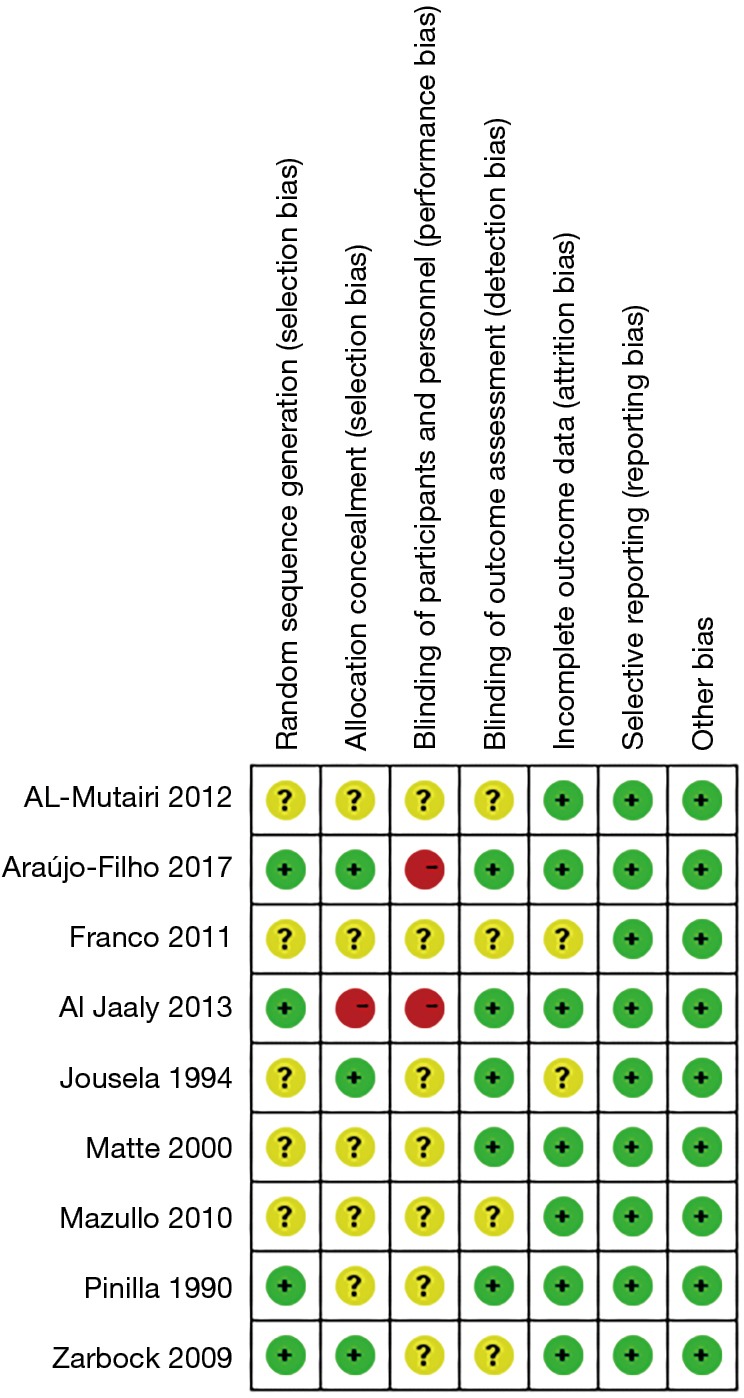
Methods: We searched PubMed, Embase, Web of Science and Cochrane Central for randomized controlled trials comparing the use of NIV (continues positive airway pressure or bi-level positive airway pressure) with standard treatment in post-cardiac surgery subjects without language restriction. Two investigators screened the eligible studies up to July, 2019. Meta-analysis using random effect model or fixed effect model was conducted for pulmonary complications, mortality, rate of reintubation and cardiac complications, and mean difference (MD) or standard mean difference for length of hospital stay and length of ICU stay.
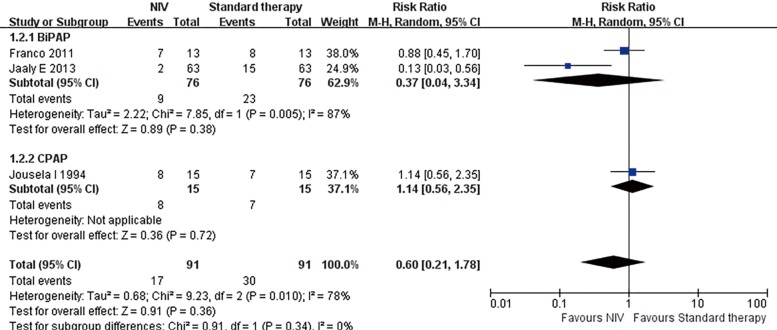
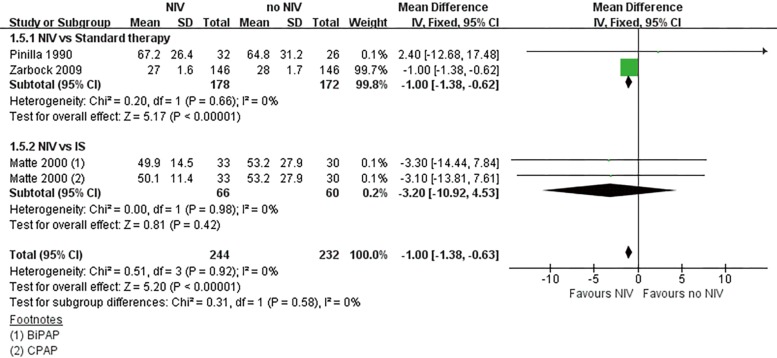
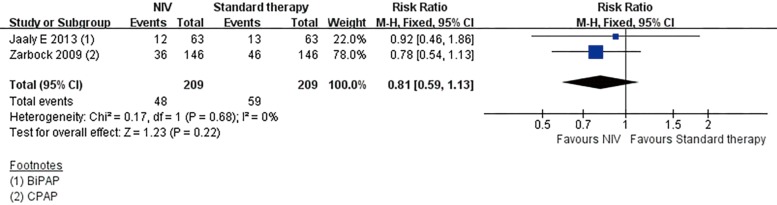
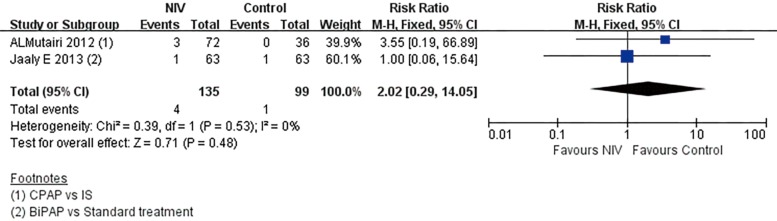
Results: We included nine randomized controlled trails with 830 subjects. The use of NIV failed to reduce the risk of pulmonary complications, including atelectasis [risk rate (RR) 0.60; 95% confidence interval (CI): 0.28 to 1.28, P=0.19] and pneumonia (RR 0.27; 95% CI: 0.05 to 1.64, P=0.16). However, it has shortened the length of ICU stay (MD -1.00 h, 95% CI: -1.38 to -0.63, P<0.00001) and the length of hospital stay (MD -1.00 d, 95% CI: -1.12 to -0.87, P<0.00001). NIV also failed to reduce the rate of reintubation (RR 0.68; 95% CI: 0.21 to 2.26, P=0.53) or the risk of cardiac complications (RR 0.81; 95% CI: 0.59 to 1.13, P=0.22).
Conclusions: The prophylactic use of NIV immediately in post-cardiac subjects who underwent cardiac surgery might be able to shorten the length of hospital stay and the length of ICU stay, but it has no significant effect on pulmonary complications, rate of reintubation or cardiac complications.
Keywords: Cardiac surgical procedure; continuous positive airway pressure (CPAP); length of stay; noninvasive ventilations; postoperative complications; pulmonary atelectasis.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd.2020.02.30). The authors have no conflicts of interest to declare.
Figures






References
-
- Gardner B, Palasti S. A comparison of hospital costs and morbidity between octogenarians and other patients undergoing general surgical operations. Surg Gynecol Obstet 1990;171:299-304. - PubMed
LinkOut - more resources
Full Text Sources