

ESHRE guideline: ovarian stimulation for IVF/ICSI†
- PMID: 32395637
- PMCID: PMC7203749
- DOI: 10.1093/hropen/hoaa009
ESHRE guideline: ovarian stimulation for IVF/ICSI†
Erratum in
-
Erratum: ESHRE guideline: ovarian stimulation for IVF/ICSI.Hum Reprod Open. 2020 Dec 29;2020(4):hoaa067. doi: 10.1093/hropen/hoaa067. eCollection 2020. Hum Reprod Open. 2020. PMID: 33409381 Free PMC article.
Abstract
Study question: What is the recommended management of ovarian stimulation, based on the best available evidence in the literature?
Summary answer: The guideline development group formulated 84 recommendations answering 18 key questions on ovarian stimulation.
What is known already: Ovarian stimulation for IVF/ICSI has been discussed briefly in the National Institute for Health and Care Excellence guideline on fertility problems, and the Royal Australian and New Zealand College of Obstetricians and Gynaecologist has published a statement on ovarian stimulation in assisted reproduction. There are, to our knowledge, no evidence-based guidelines dedicated to the process of ovarian stimulation.
Study design size duration: The guideline was developed according to the structured methodology for development of ESHRE guidelines. After formulation of key questions by a group of experts, literature searches and assessments were performed. Papers published up to 8 November 2018 and written in English were included. The critical outcomes for this guideline were efficacy in terms of cumulative live birth rate per started cycle or live birth rate per started cycle, as well as safety in terms of the rate of occurrence of moderate and/or severe ovarian hyperstimulation syndrome (OHSS).
Participants/materials setting methods: Based on the collected evidence, recommendations were formulated and discussed until consensus was reached within the guideline group. A stakeholder review was organized after finalization of the draft. The final version was approved by the guideline group and the ESHRE Executive Committee.
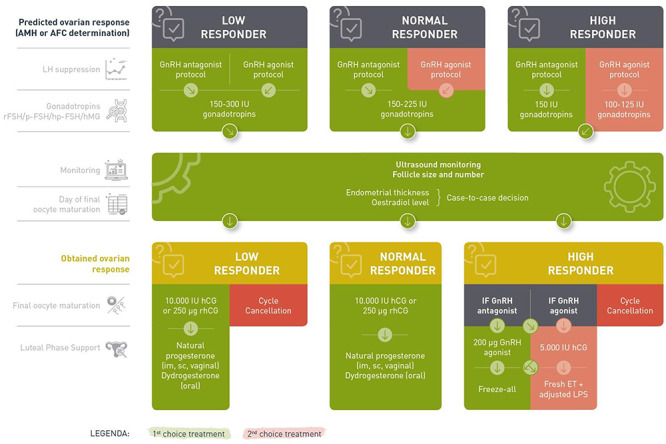
Main results and the role of chance: The guideline provides 84 recommendations: 7 recommendations on pre-stimulation management, 40 recommendations on LH suppression and gonadotrophin stimulation, 11 recommendations on monitoring during ovarian stimulation, 18 recommendations on triggering of final oocyte maturation and luteal support and 8 recommendations on the prevention of OHSS. These include 61 evidence-based recommendations-of which only 21 were formulated as strong recommendations-and 19 good practice points and 4 research-only recommendations. The guideline includes a strong recommendation for the use of either antral follicle count or anti-Müllerian hormone (instead of other ovarian reserve tests) to predict high and poor response to ovarian stimulation. The guideline also includes a strong recommendation for the use of the GnRH antagonist protocol over the GnRH agonist protocols in the general IVF/ICSI population, based on the comparable efficacy and higher safety. For predicted poor responders, GnRH antagonists and GnRH agonists are equally recommended. With regards to hormone pre-treatment and other adjuvant treatments (metformin, growth hormone (GH), testosterone, dehydroepiandrosterone, aspirin and sildenafil), the guideline group concluded that none are recommended for increasing efficacy or safety.
Limitations reason for caution: Several newer interventions are not well studied yet. For most of these interventions, a recommendation against the intervention or a research-only recommendation was formulated based on insufficient evidence. Future studies may require these recommendations to be revised.
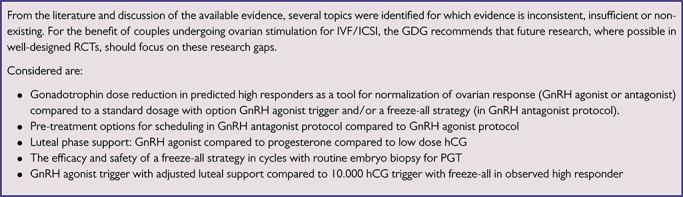
Wider implications of the findings: The guideline provides clinicians with clear advice on best practice in ovarian stimulation, based on the best evidence available. In addition, a list of research recommendations is provided to promote further studies in ovarian stimulation.
Study funding/competing interests: The guideline was developed and funded by ESHRE, covering expenses associated with the guideline meetings, with the literature searches and with the dissemination of the guideline. The guideline group members did not receive payment. F.B. reports research grant from Ferring and consulting fees from Merck, Ferring, Gedeon Richter and speaker's fees from Merck. N.P. reports research grants from Ferring, MSD, Roche Diagnositics, Theramex and Besins Healthcare; consulting fees from MSD, Ferring and IBSA; and speaker's fees from Ferring, MSD, Merck Serono, IBSA, Theramex, Besins Healthcare, Gedeon Richter and Roche Diagnostics. A.L.M reports research grants from Ferring, MSD, IBSA, Merck Serono, Gedeon Richter and TEVA and consulting fees from Roche, Beckman-Coulter. G.G. reports consulting fees from MSD, Ferring, Merck Serono, IBSA, Finox, Theramex, Gedeon-Richter, Glycotope, Abbott, Vitrolife, Biosilu, ReprodWissen, Obseva and PregLem and speaker's fees from MSD, Ferring, Merck Serono, IBSA, Finox, TEVA, Gedeon Richter, Glycotope, Abbott, Vitrolife and Biosilu. E.B. reports research grants from Gedeon Richter; consulting and speaker's fees from MSD, Ferring, Abbot, Gedeon Richter, Merck Serono, Roche Diagnostics and IBSA; and ownership interest from IVI-RMS Valencia. P.H. reports research grants from Gedeon Richter, Merck, IBSA and Ferring and speaker's fees from MSD, IBSA, Merck and Gedeon Richter. J.U. reports speaker's fees from IBSA and Ferring. N.M. reports research grants from MSD, Merck and IBSA; consulting fees from MSD, Merck, IBSA and Ferring and speaker's fees from MSD, Merck, IBSA, Gedeon Richter and Theramex. M.G. reports speaker's fees from Merck Serono, Ferring, Gedeon Richter and MSD. S.K.S. reports speaker's fees from Merck, MSD, Ferring and Pharmasure. E.K. reports speaker's fees from Merck Serono, Angellini Pharma and MSD. M.K. reports speaker's fees from Ferring. T.T. reports speaker's fees from Merck, MSD and MLD. The other authors report no conflicts of interest.
Disclaimer: This guideline represents the views of ESHRE, which were achieved after careful consideration of the scientific evidence available at the time of preparation. In the absence of scientific evidence on certain aspects, a consensus between the relevant ESHRE stakeholders has been obtained. Adherence to these clinical practice guidelines does not guarantee a successful or specific outcome, nor does it establish a standard of care. Clinical practice guidelines do not replace the need for application of clinical judgment to each individual presentation, nor variations based on locality and facility type. ESHRE makes no warranty, express or implied, regarding the clinical practice guidelines and specifically excludes any warranties of merchantability and fitness for a particular use or purpose. (Full disclaimer available at www.eshre.eu/guidelines.) †ESHRE Pages content is not externally peer reviewed. The manuscript has been approved by the Executive Committee of ESHRE.
Keywords: ESHRE; GRADE; evidence based; guideline; high responder; ovarian hyperstimulation syndrome; ovarian stimulation; poor responder; treatment.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology.
Figures
Comment in
-
Questionable recommendation for LPS for IVF/ICSI in ESHRE guideline 2019: ovarian stimulation for IVF/ICSI.Hum Reprod Open. 2021 Mar 3;2021(1):hoab005. doi: 10.1093/hropen/hoab005. eCollection 2021. Hum Reprod Open. 2021. PMID: 33718622 Free PMC article. No abstract available.
-
Reply: Questionable recommendation for LPS for IVF/ICSI in ESHRE guideline 2019: ovarian stimulation for IVF/ICSI.Hum Reprod Open. 2021 Mar 3;2021(1):hoab006. doi: 10.1093/hropen/hoab006. eCollection 2021. Hum Reprod Open. 2021. PMID: 33718623 Free PMC article. No abstract available.
References
-
- Aboulghar MA, Mansour RT, Serour GI, Al-Inany HG, Amin YM, Aboulghar MM. Increasing the dose of human menopausal gonadotrophins on day of GnRH antagonist administration: randomized controlled trial. Reprod Biomed Online 2004;8:524–527. - PubMed
-
- Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y, Nasser M, Meerpohl J, Post PN, Kunz R et al. . GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol 2013;66:719–725. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials