

Effect of Surgery vs Functional Bracing on Functional Outcome Among Patients With Closed Displaced Humeral Shaft Fractures: The FISH Randomized Clinical Trial
- PMID: 32396179
- PMCID: PMC7218498
- DOI: 10.1001/jama.2020.3182
Effect of Surgery vs Functional Bracing on Functional Outcome Among Patients With Closed Displaced Humeral Shaft Fractures: The FISH Randomized Clinical Trial
Abstract
Importance: Humeral shaft fractures traditionally have been treated nonsurgically, but there has been a steady increase in the rate of surgery over the past 2 decades without high-quality evidence to justify the trend.
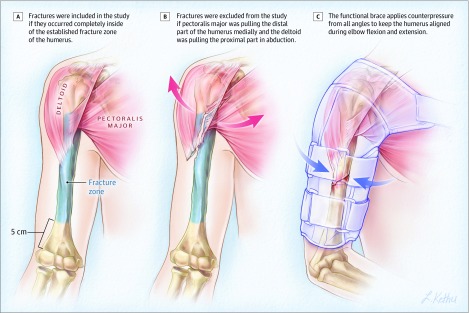
Objective: To compare the effectiveness of surgical treatment with open reduction and internal plate fixation to nonsurgical treatment with functional bracing in the treatment of closed humeral shaft fractures.
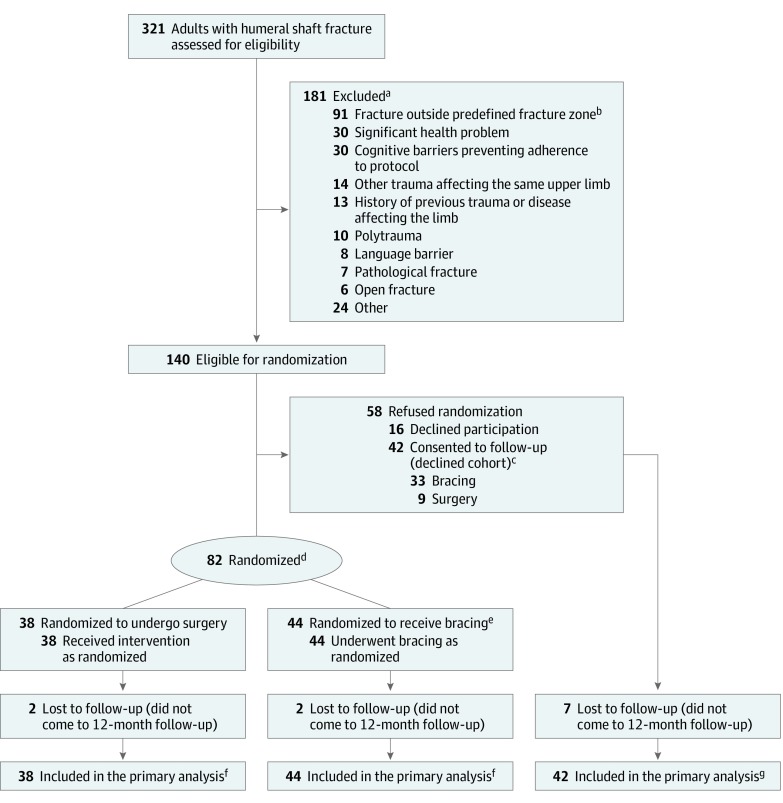
Design, setting, and participants: Randomized clinical trial conducted at 2 university hospital trauma centers in Finland, enrollment between November 2012 and January 2018 with a final follow-up of January 2019. A total of 82 adult patients with closed, unilateral, displaced humeral shaft fracture met criteria for inclusion. Patients were excluded if they had cognitive disabilities preventing them from following the protocol or had multimorbidity or multiple trauma.
Interventions: Patients were randomly assigned to surgical treatment with open reduction and internal plate fixation (n = 38) or to nonsurgical treatment with functional bracing (n = 44).
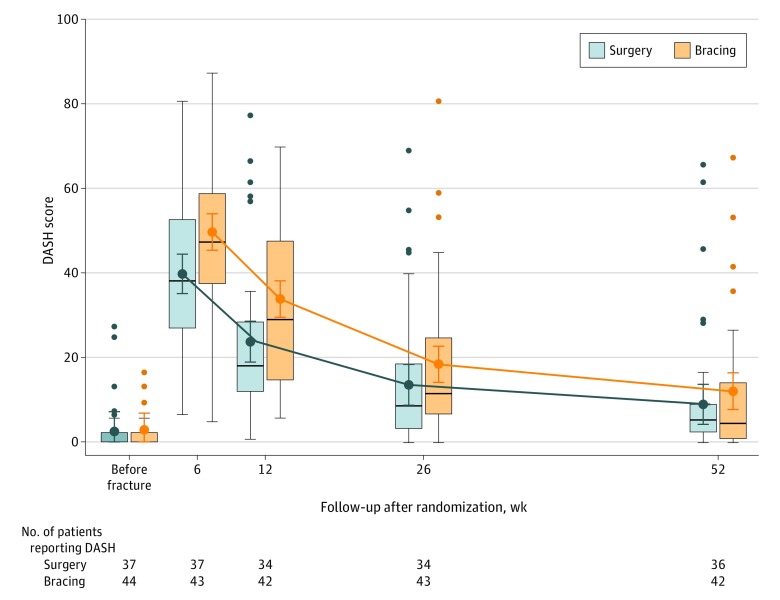
Main outcome and measure: The primary outcome was Disabilities of Arm, Shoulder and Hand (DASH) score at 12 months (range, 0 to 100 points, 0 denotes no disability and 100 extreme disability; minimal clinically important difference, 10 points).
Results: Among 82 patients who were randomized (mean age, 48.9 years; 38 women [46%]; 44 men [54%]), 78 (95%) completed the trial. Thirteen (30%) of the patients assigned to functional bracing underwent surgery during the 12-month follow-up period to promote healing of the fracture. At 12 months, the mean DASH score was 8.9 (95% CI, 4.2 to 13.6) in the surgery group and 12.0 (95% CI, 7.7 to 16.4) in the bracing group (between-group difference, -3.1 points; 95% CI, -9.6 to 3.3; P = .34). Eleven patients (25%) allocated to functional bracing developed fracture nonunion. Three patients (8%) allocated to surgery developed a temporary radial nerve palsy.
Conclusions and relevance: Among patients with closed humeral shaft fracture, internal fixation surgery, compared with nonoperative functional bracing, did not significantly improve functional outcomes at 12 months. However, the substantial amount of treatment crossover from nonoperative to surgical treatment should be considered when interpreting the trial results.
Trial registration: ClinicalTrials.gov Identifier: NCT01719887.
Conflict of interest statement
Figures
Comment in
-
In Closed Humeral Shaft Fractures, Internal Fixation Surgery Did Not Improve Functional Outcomes at 12 Months Compared with Nonoperative Functional Bracing.J Bone Joint Surg Am. 2021 Feb 17;103(4):356. doi: 10.2106/JBJS.20.02087. J Bone Joint Surg Am. 2021. PMID: 33369986 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
