

Comparing transplant outcomes in ALL patients after haploidentical with PTCy or matched unrelated donor transplantation
- PMID: 32396617
- PMCID: PMC7218425
- DOI: 10.1182/bloodadvances.2020001499
Comparing transplant outcomes in ALL patients after haploidentical with PTCy or matched unrelated donor transplantation
Abstract
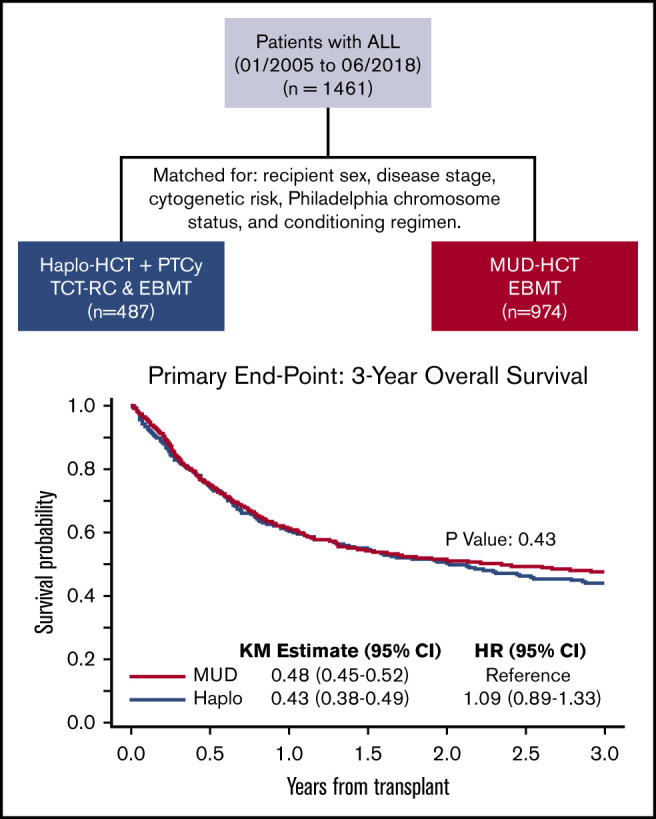
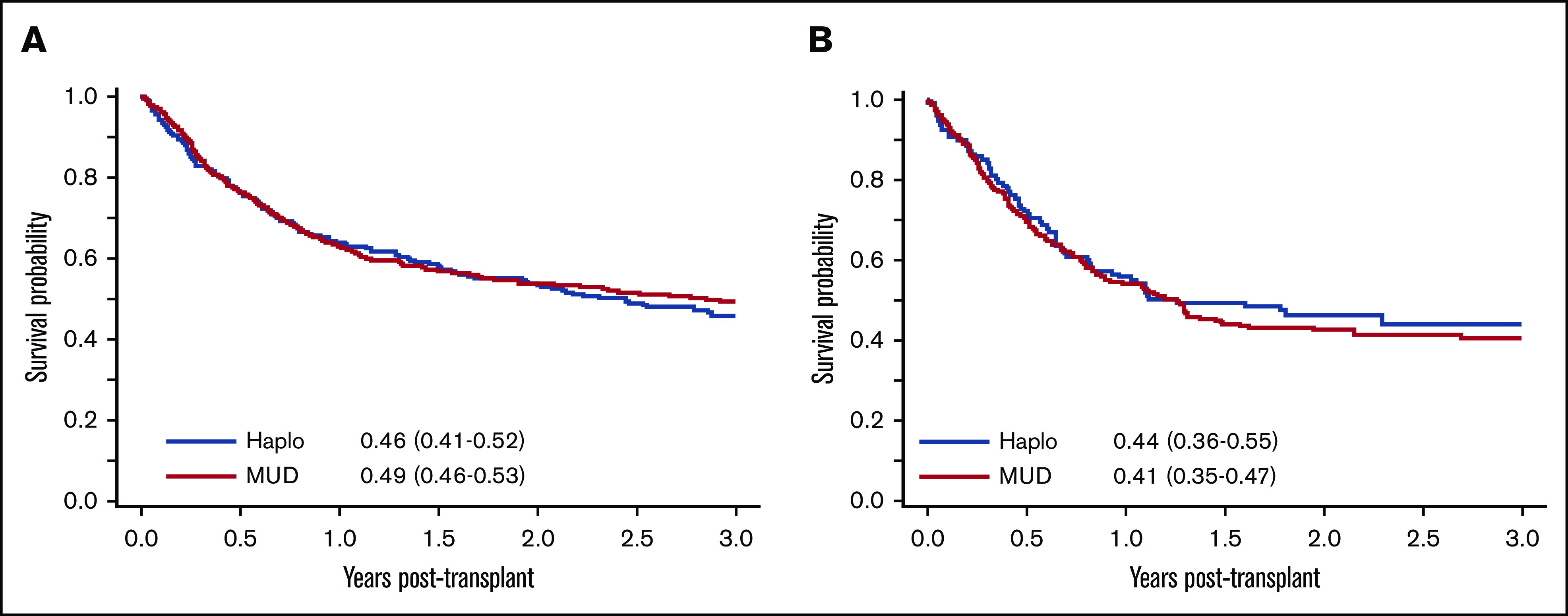
We compared outcomes of 1461 adult patients with acute lymphoblastic leukemia (ALL) receiving hematopoietic cell transplantation (HCT) from a haploidentical (n = 487) or matched unrelated donor (MUD; n = 974) between January 2005 and June 2018. Graft-versus-host disease (GVHD) prophylaxis was posttransplant cyclophosphamide (PTCy), calcineurin inhibitor (CNI), and mycophenolate mofetil (MMF) for haploidentical, and CNI with MMF or methotrexate with/without antithymoglobulin for MUDs. Haploidentical recipients were matched (1:2 ratio) with MUD controls for sex, conditioning intensity, disease stage, Philadelphia-chromosome status, and cytogenetic risk. In the myeloablative setting, day +28 neutrophil recovery was similar between haploidentical (87%) and MUD (88%) (P = .11). Corresponding rates after reduced-intensity conditioning (RIC) were 84% and 88% (P = .47). The 3-month incidence of grade II-IV acute GVHD (aGVHD) and 3-year chronic GVHD (cGVHD) was similar after haploidentical compared with MUD: myeloablative conditioning, 33% vs 34% (P = .46) for aGVHD and 29% vs 31% for cGVHD (P = .58); RIC, 31% vs 30% (P = .06) for aGVHD and 24% vs 29% for cGVHD (P = .86). Among patients receiving myeloablative regimens, 3-year probabilities of overall survival were 44% and 51% with haploidentical and MUD (P = .56). Corresponding rates after RIC were 43% and 42% (P = .6). In this large multicenter case-matched retrospective analysis, despite the limitations of a registry-based study (ie, unavailability of key elements such as minimal residual disease testing), our analysis indicated that outcomes of patients with ALL undergoing HCT from a haploidentical donor were comparable with 8 of 8 MUD transplantations.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Cornelissen JJ, van der Holt B, Verhoef GE, et al. ; Dutch-Belgian HOVON Cooperative Group . Myeloablative allogeneic versus autologous stem cell transplantation in adult patients with acute lymphoblastic leukemia in first remission: a prospective sibling donor versus no-donor comparison. Blood. 2009;113(6):1375-1382. - PubMed
-
- Fielding AK, Richards SM, Chopra R, et al. ; Eastern Cooperative Oncology Group . Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109(3):944-950. - PubMed
-
- Goldstone AH, Richards SM, Lazarus HM, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993). Blood. 2008;111(4):1827-1833. - PubMed
-
- Thomas X, Boiron JM, Huguet F, et al. Outcome of treatment in adults with acute lymphoblastic leukemia: analysis of the LALA-94 trial. J Clin Oncol. 2004;22(20):4075-4086. - PubMed
-
- Lee S, Cho B-S, Kim S-Y, et al. Allogeneic stem cell transplantation in first complete remission enhances graft-versus-leukemia effect in adults with acute lymphoblastic leukemia: antileukemic activity of chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2007;13(9):1083-1094. - PubMed
