

Single-Cell Transcriptome Analysis Reveals Intratumoral Heterogeneity in ccRCC, which Results in Different Clinical Outcomes
- PMID: 32396851
- PMCID: PMC7335756
- DOI: 10.1016/j.ymthe.2020.04.023
Single-Cell Transcriptome Analysis Reveals Intratumoral Heterogeneity in ccRCC, which Results in Different Clinical Outcomes
Abstract
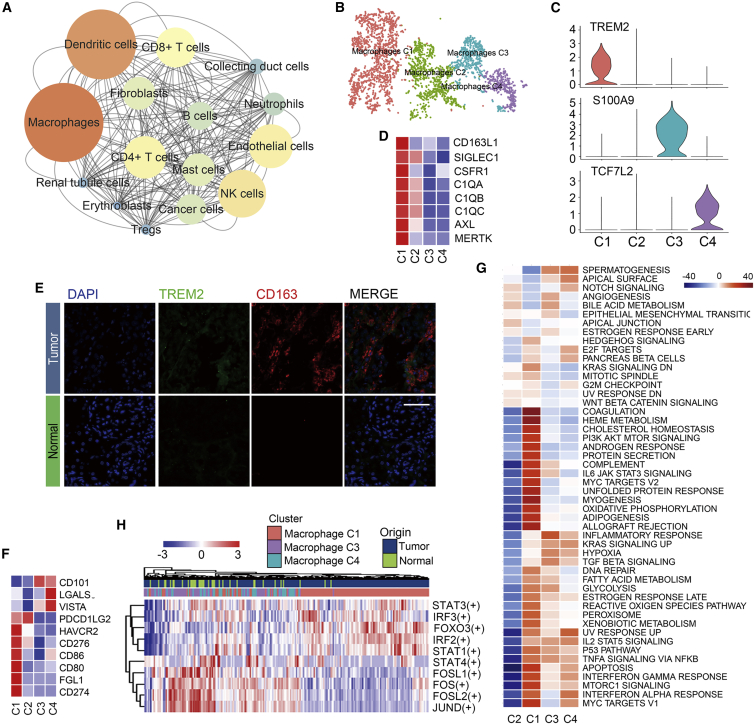
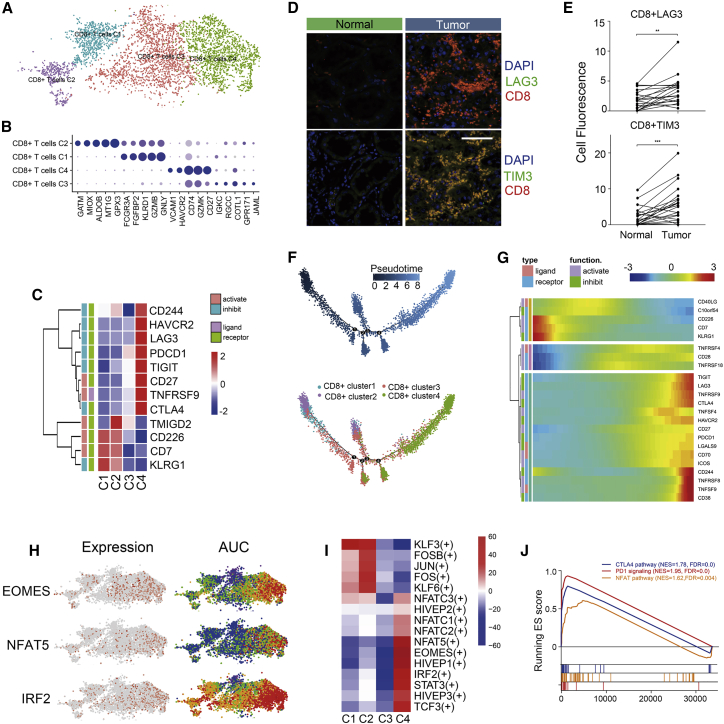
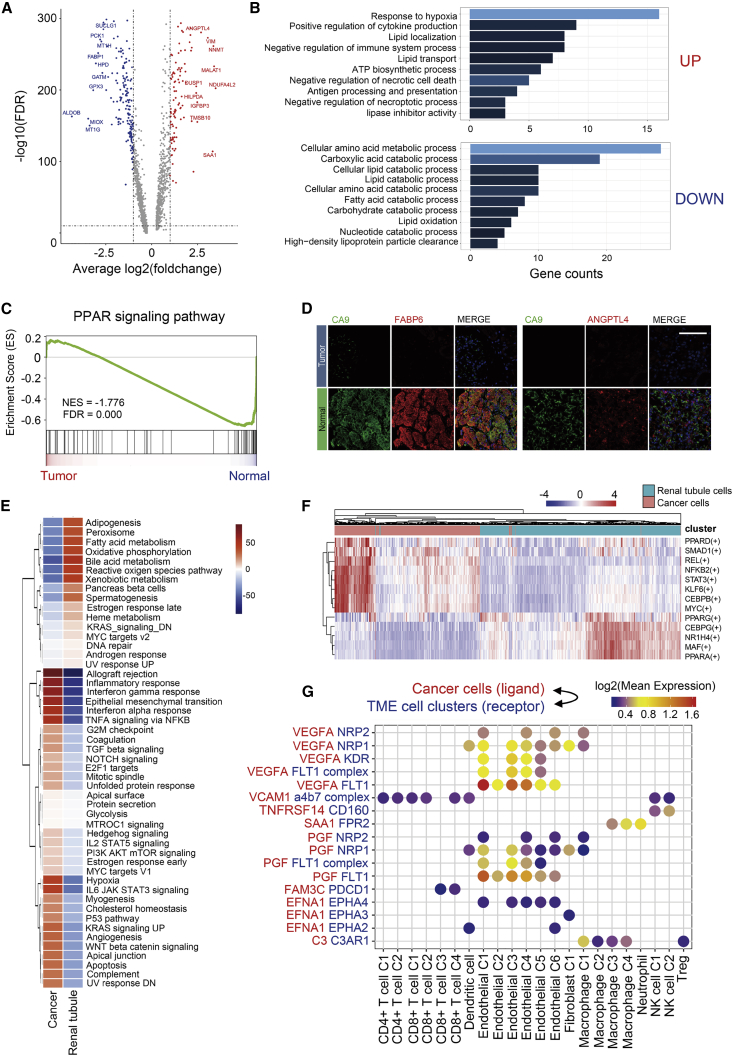
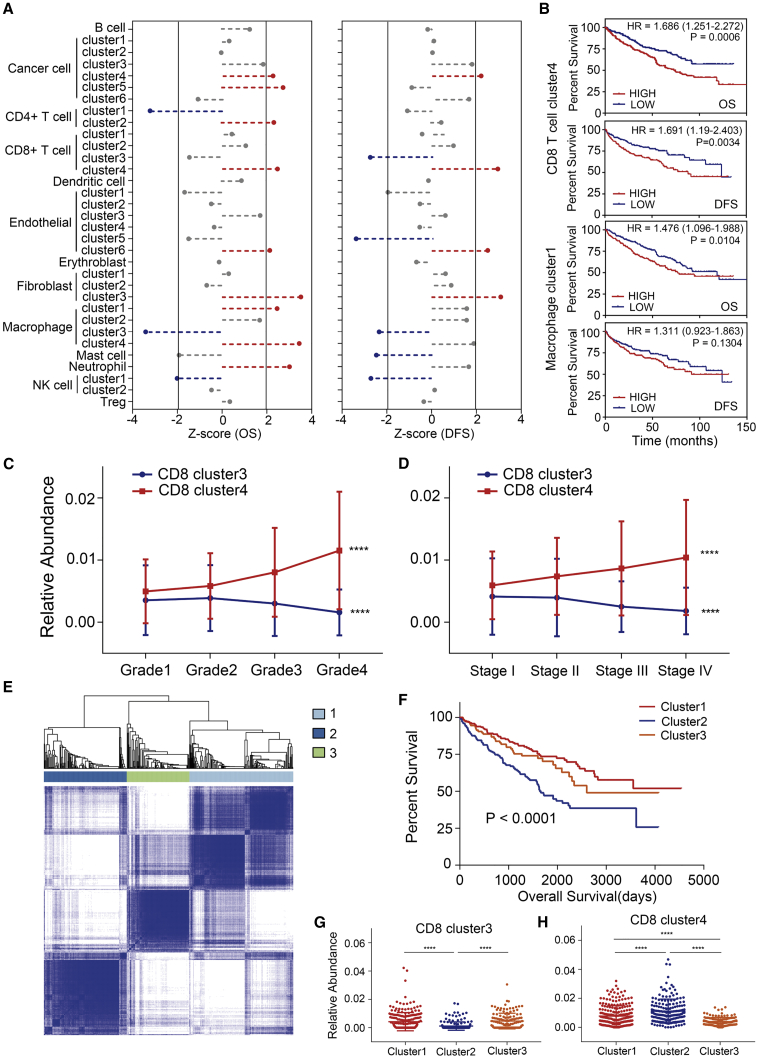
Clear-cell renal cell carcinoma (ccRCC) is the most common histological type of RCC. To investigate the intratumoral heterogeneity of ccRCC, we analyzed single-cell RNA-sequencing data and identified 15 major cell types, along with 39 subgroups of cells derived from tumor or non-malignant tissues, and confirmed their presence by immunofluorescence staining in tissue chips. In this study, we verified that T cell exhaustion was the key factor responsible for the immunosuppressive property of ccRCC tissues, which was significantly related to poor prognosis. We also found that abnormal metabolic patterns occurred not only in cancer cells, but also in tumor-infiltrating stromal cells. Based on the fraction of each cell cluster detected by CIBERSORTx, 533 patients from The Cancer Genome Atlas (TCGA) KIRC dataset were divided into three groups. One group, which showed a lesser proportion of activated CD8+ cells and greater proportion of exhausted CD8+ cells, was associated with a poor prognosis. Hence, the blockade of immunosuppressive checkpoints, not only PD-1, but also LAG3, TIM-3, and other inhibitory checkpoints, could serve as a potential target for ccRCC immunotherapy. Our work will further the understanding of the heterogeneity among ccRCC tissues and provide novel strategies for treating ccRCC.
Keywords: T cell exhaustion; bioinformatics; clear-cell renal cell carcinoma; heterogeneity; single-cell sequencing; tumor microenvironment.
Copyright © 2020 The American Society of Gene and Cell Therapy. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68:394–424. - PubMed
-
- Porta C., Cosmai L., Leibovich B.C., Powles T., Gallieni M., Bex A. The adjuvant treatment of kidney cancer: a multidisciplinary outlook. Nat. Rev. Nephrol. 2019;15:423–433. - PubMed
-
- Grimm M.O., Bex A., De Santis M., Ljungberg B., Catto J.W.F., Rouprêt M., Hussain S.A., Bellmunt J., Powles T., Wirth M., Van Poppel H. Safe use of immune checkpoint inhibitors in the multidisciplinary management of urological cancer: the European Association of Urology position in 2019. Eur. Urol. 2019;76:368–380. - PubMed
-
- Kotecha R.R., Motzer R.J., Voss M.H. Towards individualized therapy for metastatic renal cell carcinoma. Nat. Rev. Clin. Oncol. 2019;16:621–633. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
