

High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation
- PMID: 32397087
- PMCID: PMC7277091
- DOI: 10.3390/antibiotics9050237
High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation
Abstract
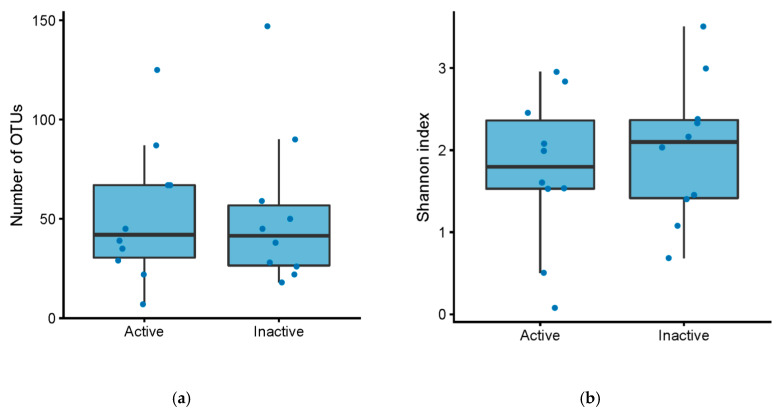
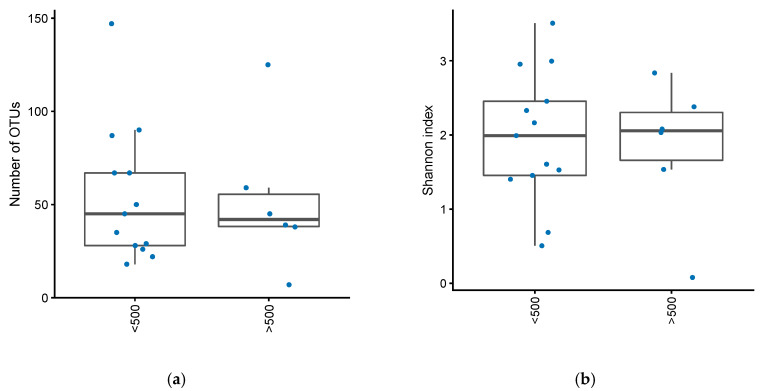
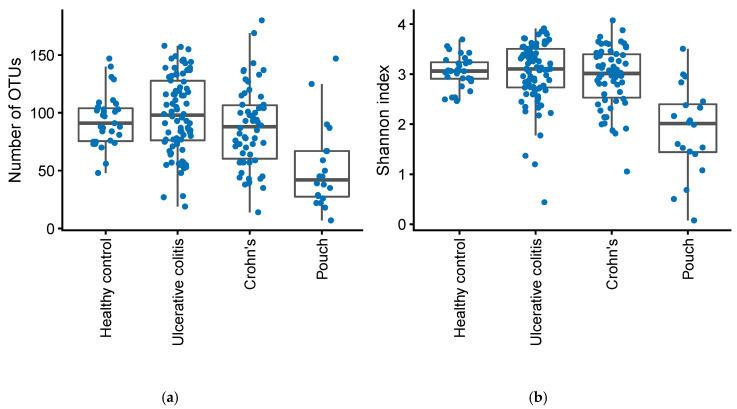
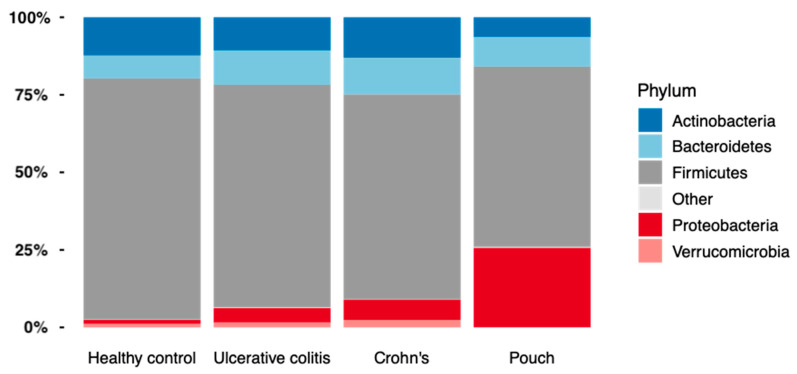
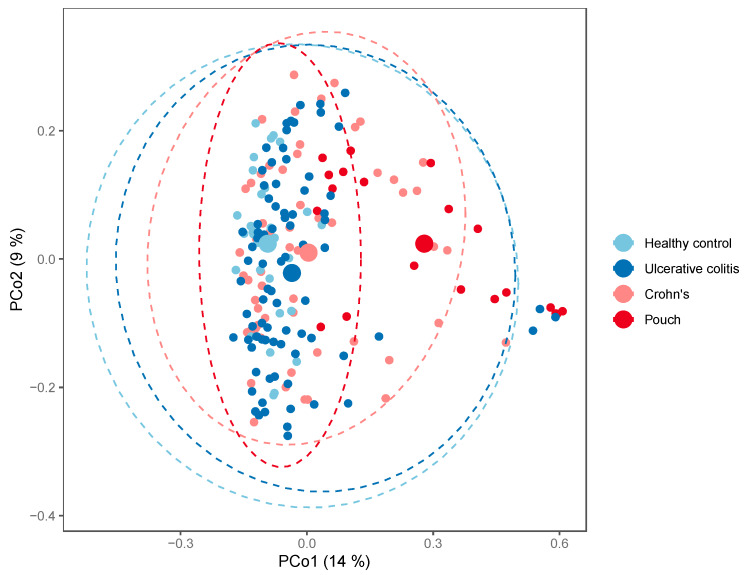
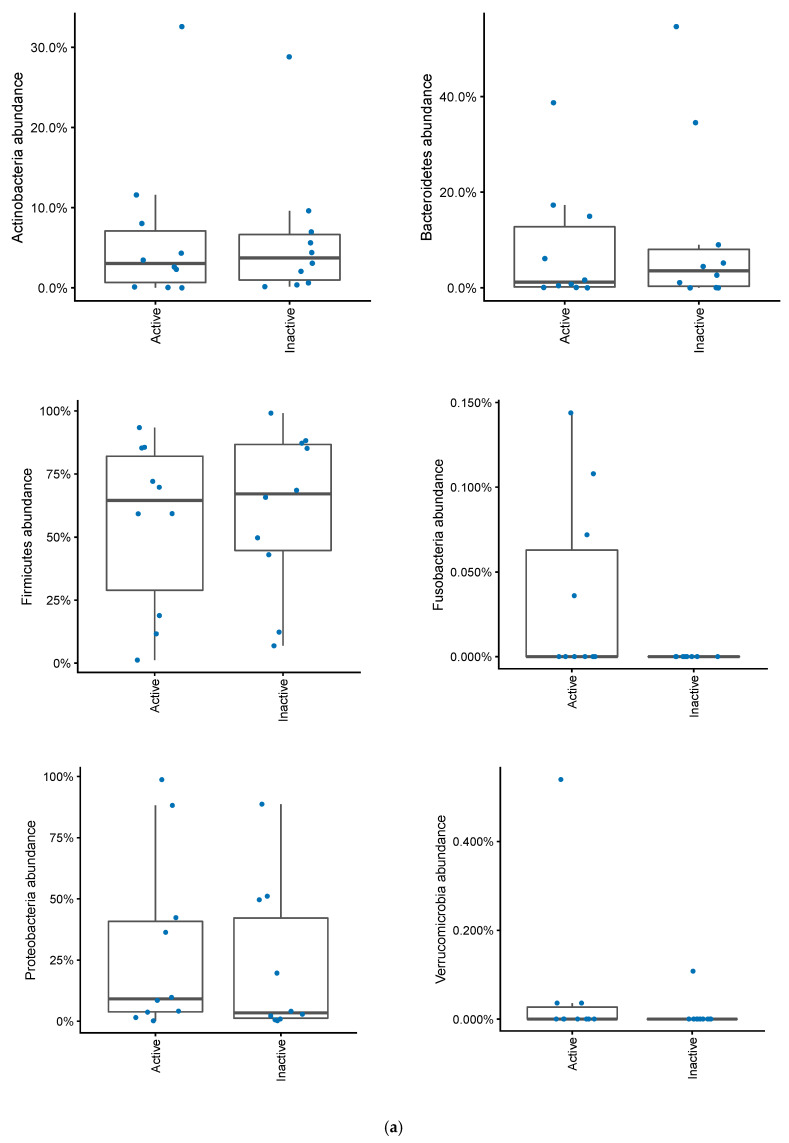
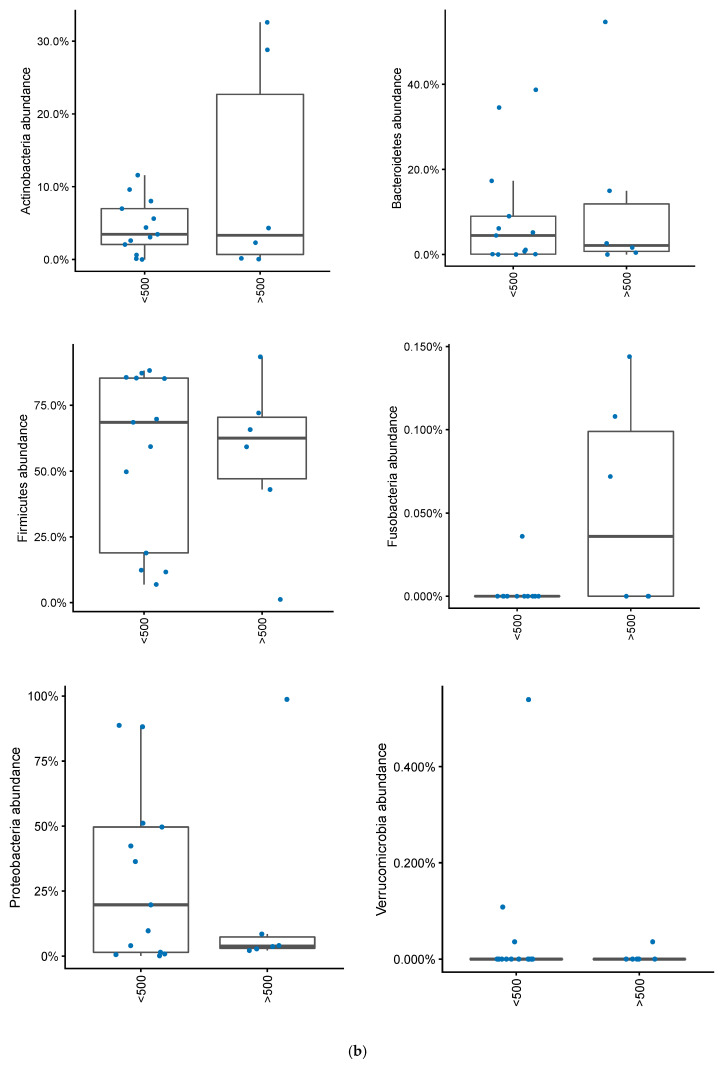
Low diversity intestinal dysbiosis has been associated with inflammatory bowel disease, including patients with ulcerative colitis with an ileo-anal pouch anastomosis. Furthermore, specific Escherichia coli phylogroups have been linked to inflammatory bowel disease. Our aim was to characterize the differences among microbiota and E. coli phylogroups in active and inactive pouchitis. Disease activity was assessed using the modified pouch disease activity index and by fecal calprotectin. Microbiota diversity was assessed by 16S rDNA MiSeq sequencing. E. coli phylogroup was determined after triplex PCR. Twenty patients with ulcerative colitis with an ileo-anal pouch anastomosis were included, 10 of whom had active pouchitis. Ileo-anal pouch anastomosis patients had an increased abundance of Proteobacteria colonization compared to patients with ulcerative colitis or Crohn's disease and healthy controls, p = 1.4·10-5. No differences in E. coli phylogroup colonization could be determined between cases of active and inactive disease. No significant link was found between α-diversity and pouch inflammation. However, higher levels of Fusobacteria colonization were found in patients with a pouch with a fecal calprotectin level above 500, p = 0.02. In conclusion, patients with a pouch had an increased Proteobacteria abundance, but only Fusobacteria abundance was linked to inflammation.
Keywords: Escherichia coli; Fusobacteria; Proteobacteria; calprotectin; inflammatory bowel disease; pouchitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
